Loading
Get Member Self-pay Reimbursement Form
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the MEMBER SELF-PAY REIMBURSEMENT FORM online
Filling out the MEMBER SELF-PAY REIMBURSEMENT FORM online can enhance your experience in obtaining reimbursements for your self-paid medical expenses. This guide will provide you with clear and accessible instructions to ensure you complete the form accurately and efficiently.
Follow the steps to successfully complete the reimbursement form
- Click ‘Get Form’ button to obtain the form and open it in your preferred editor.
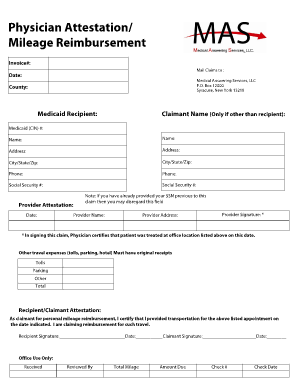
- Enter the invoice number in the designated field at the top of the form to ensure proper processing of your claim.
- Fill in the date when you are completing the form. This helps establish the timeline of your claim.
- Provide the name and address of Medical Answering Services, LLC as indicated on the form: P.O. Box 12000, Syracuse, New York 13218.
- In the county field, specify the county where the services were rendered.
- Enter the Medicaid recipient's name and their associated Medicaid (CIN) number in the designated fields.
- Include the address, city, state, and zip code of the recipient for accurate identification.
- Provide the phone number and Social Security number of the recipient.
- For provider attestation, enter the provider's name, address, and date of service.
- The provider must sign the document to certify that the patient received treatment on the specified date.
- If applicable, list any other travel expenses such as tolls, parking, and hotel accommodations. Original receipts are required for these expenses.
- Include the total amounts for all claimed expenses to summarize your reimbursement request.
- As the recipient or claimant, sign and date the attestation to confirm that you provided transportation for the listed appointment.
- Finalize the form by saving changes, downloading a copy, printing it for your records, or sharing it as needed.
Complete your MEMBER SELF-PAY REIMBURSEMENT FORM online today to ensure you receive the reimbursements you deserve.
It is used in the healthcare industry to submit insurance claims to Medicare or other health insurance companies. Completion of this form helps insurance companies decide whether the healthcare provider should receive reimbursement.