Loading
Get Fillable Wellcare Form
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the Fillable Wellcare Form online
Filling out the Fillable Wellcare Form online can be straightforward if you understand the process. This guide provides clear, step-by-step instructions to ensure you complete the form accurately and efficiently.
Follow the steps to successfully fill out the Fillable Wellcare Form online.
- Click ‘Get Form’ button to obtain the Fillable Wellcare Form and open it in your preferred online editor.
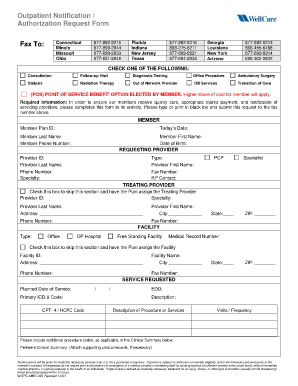
- In the required information section, enter the member's Plan ID, today's date, last name, phone number, first name, and date of birth. Ensure all fields are completed clearly.
- Next, move to the requesting provider section. Input the provider's ID, last name, phone number, specialty, first name, and fax number in the designated fields.
- For the treating provider section, you have the option to skip it or enter the treating provider's ID, specialty, last name, phone number, address, city, state, ZIP code, and fax number as needed.
- Proceed to the facility information. Check the box to skip this section or fill in the facility ID, address, phone number, planned date of service, primary ICD-9 code, CPT-4 / HCPC code, facility name, city, state, ZIP code, and fax number.
- In the service requested section, specify the description of the procedure or services needed, visits, frequency, and include any additional procedure codes in the clinical summary.
- Review your completed form to ensure all information is accurate and complete. If any attachments are necessary, make sure they are included.
- Finally, save your changes, download the completed form, print it, or share it as required. You may also send it to the appropriate fax number listed on the form.
Complete your documents online for quicker processing and efficient management.
Claims Department PO Box 31224 Tampa, FL 33631-3224 The Claim Payment Dispute process is designed to address claims when there is disagreement regarding reimbursement. Claim payment disputes must be submitted to WellCare in writing within 90 days of the date of denial on the EOP.
Industry-leading security and compliance
US Legal Forms protects your data by complying with industry-specific security standards.
-
In businnes since 199725+ years providing professional legal documents.
-
Accredited businessGuarantees that a business meets BBB accreditation standards in the US and Canada.
-
Secured by BraintreeValidated Level 1 PCI DSS compliant payment gateway that accepts most major credit and debit card brands from across the globe.