Loading
Get Mn Fr01 Form
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the Mn Fr01 Form online
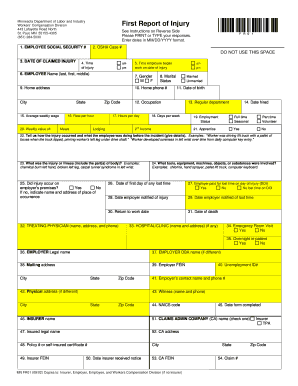
Filling out the Mn Fr01 Form online is essential for reporting work-related injuries to ensure proper processing and support. This guide will provide you with clear and concise steps to successfully complete the form, making the process straightforward for all users.
Follow the steps to fill out the Mn Fr01 Form online:
- Press the ‘Get Form’ button to access the Mn Fr01 Form and open it in your selected editor.
- Begin by entering the employee's social security number in the designated field. Be sure to enter the number accurately to avoid delays.
- Next, fill in the OSHA Case number if applicable. Leave this field blank if not relevant.
- In the section for the date of the claimed injury, use the MM/DD/YYYY format to ensure clarity.
- Indicate the time of injury, selecting either AM or PM as appropriate.
- Enter the time the employee began work on the date of the injury, again selecting AM or PM.
- Provide the employee's full name — last, first, and middle — in the specified fields.
- Select the employee's gender by marking the appropriate box.
- Fill in the employee's home address, including the city, state, and zip code.
- State the employee's average weekly wage along with the rate per hour.
- In the subsequent fields, provide information about the employee's marital status and date of birth.
- Specify the employee's occupation and regular department they work in.
- Enter the date the employee was hired.
- Determine the employment status by checking the relevant option: full-time, part-time, seasonal, volunteer.
- Indicate if the employee is an apprentice by selecting yes or no.
- Describe how the injury occurred in detail, including what the employee was doing at the time of the injury.
- Specify the nature of the injury or illness, giving details on the affected body part(s).
- Indicate whether the injury occurred on the employer's premises and provide relevant details if it did not.
- List any tools, equipment, or substances involved in the incident.
- Fill in the date of the first day of any lost time due to the injury.
- Mark whether the employer paid for lost time on the day of the injury.
- Provide the dates the employer was notified of the injury and of any lost time.
- Indicate the planned return to work date, if applicable.
- If relevant, provide the date of death.
- Fill in the treating physician's name, address, and phone number.
- List the hospital or clinic's name and address, if applicable.
- Specify if there was an emergency room visit or if the employee was an overnight in-patient.
- Complete the employer's legal name, DBA name if different, mailing address, and FEIN.
- Provide the employer's contact name and phone number.
- If applicable, fill in the witness's name and phone number.
- Include the employer's NAICS code.
- Record the date the form is completed.
- Provide the insurer's name, the insured's legal name, policy number or self-insured certificate, and their FEIN.
- Indicate the claims administration company's name, address, and FEIN if applicable.
- After ensuring all information is complete and accurate, users can save changes, download, print, or share the form.
Complete your Mn Fr01 Form online today to ensure efficient processing of your workers' compensation claim.
Going from and coming to work Normally, injuries incurred during regular commutes to and from work are not covered by workers' compensation as the time spent and act of commuting is not part of the scope and course of employment. This is called the going-and-coming rule.