Loading
Get P Roof Of Representation Authorized Representative
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the P ROOF OF REPRESENTATION Authorized Representative online
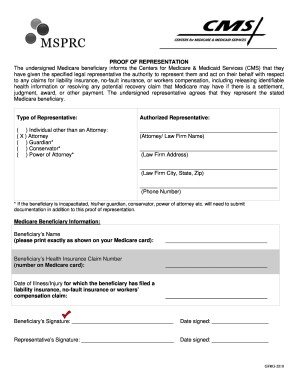
Filling out the P ROOF OF REPRESENTATION Authorized Representative form is a crucial step in designating someone to act on your behalf with respect to Medicare claims. This guide provides clear, step-by-step instructions to help you complete the form accurately and effectively.
Follow the steps to complete the form successfully.
- Press the ‘Get Form’ button to access the form and open it in your preferred online editing tool.
- Identify the section for authorized representatives. Here, you will specify who is representing you, including options such as attorney or guardian. Make sure to select the appropriate category.
- Enter the name of the authorized representative or law firm in the designated field. Ensure that all information is accurate and complete.
- Complete the representative's address, including street, city, state, and zip code, to ensure proper communication.
- Fill in the representative's phone number to facilitate any necessary contact regarding your claims.
- Provide your information as a Medicare beneficiary. Type your name exactly as it appears on your Medicare card.
- Input your Health Insurance Claim Number, which can be found on your Medicare card.
- Record the date of the illness or injury for which you are filing a claim. This information is essential for processing your representation.
- Sign and date the form as the Medicare beneficiary. This confirms that you authorize the designated representative.
- Ensure the authorized representative also signs and dates the form. Their signature is required to validate the representation.
- Once all sections are complete, you can save changes, download, print, or share the form as needed.
Complete the P ROOF OF REPRESENTATION Authorized Representative form online today to ensure proper representation for your Medicare claims.
Proof of Representation is required for the Benefits Coordination & Recovery Center (BCRC) to communicate with and provide information to an attorney that represents a Medicare beneficiary.
Industry-leading security and compliance
US Legal Forms protects your data by complying with industry-specific security standards.
-
In businnes since 199725+ years providing professional legal documents.
-
Accredited businessGuarantees that a business meets BBB accreditation standards in the US and Canada.
-
Secured by BraintreeValidated Level 1 PCI DSS compliant payment gateway that accepts most major credit and debit card brands from across the globe.