Loading
Get Medical Justification Form
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the Medical Justification Form online
Completing the Medical Justification Form online is a crucial step in securing necessary medical equipment and supports for individuals enrolled in various programs. This guide provides a clear and detailed breakdown of each section to help you navigate the process smoothly.
Follow the steps to expertly complete the Medical Justification Form.
- Press the ‘Get Form’ button to retrieve the Medical Justification Form and open it in the online editor.
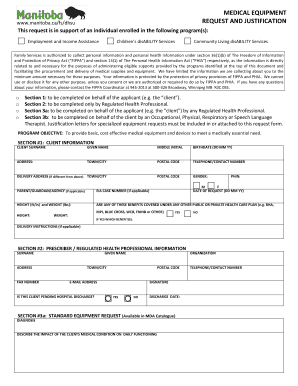
- Begin with Section 1, which requires client information. Fill in the client’s surname, given name, and middle initial, followed by their birthdate, address, town or city, postal code, and telephone number. If applicable, provide a delivery address and the client’s gender. Include the Personal Health Identification Number (PHIN) along with the date of request, and if relevant, the parent, guardian, or agency details and EIA case number.
- Section 2 is designated for entry by a regulated health professional. They need to fill out their surname, given name, and contact details, including fax number, email address, and whether the client is pending hospital discharge. A signature and discharge date should also be provided.
- In Section 3a, the regulated health professional must describe the diagnosis and its impact on the client's daily functioning. They should then specify the medical equipment requested using the MDA Catalogue products, including the SAP number and quantity.
- Section 3b is for specialized equipment requests. A justification letter or report must accompany this request. Detail the diagnosis, assess the client’s functional status, and document any relevant medical interventions. Address environmental factors, equipment trials, and the expected outcomes for the requested devices.
- Review all sections thoroughly to ensure accuracy and completeness. Once satisfied with the entries, save your changes. You can then download, print, or share the completed Medical Justification Form as necessary.
Take the first step toward accessing essential medical supports by completing your Medical Justification Form online today.
A certificate of medically necessity (CMN) is documentation from a doctor which Medicare requires before it will cover certain durable medical equipment (DME). The CMN states the patient's diagnosis, prognosis, reason for the equipment, and estimated duration of need.