Loading
Get Medicare Reconsideration Form
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the Medicare Reconsideration Form online
Filling out the Medicare Reconsideration Form online is a straightforward process that enables individuals to request a review of a claim determination. This guide offers comprehensive instructions to ensure users can accurately complete the form and submit their requests effectively.
Follow the steps to fill out the form correctly
- Click ‘Get Form’ button to obtain the form and open it for filling.
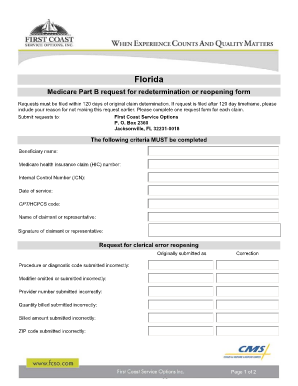
- Enter the beneficiary name clearly in the designated field. This identifies the person receiving Medicare benefits.
- Provide the Medicare health insurance claim (HIC) number. This unique identifier is essential for processing your request.
- Include the internal control number (ICN) associated with your original claim, as this helps track the claim effectively.
- Fill out the date of service when the medical services were provided. Accurate dates are crucial for determining eligibility.
- Indicate the CPT/HCPCS code for the services in question. This coding helps clarify the nature of the service provided.
- Enter the name of the claimant or representative who is submitting the request. This could be the beneficiary or a designated person.
- Sign the form in the appropriate field to validate the submission. If a representative is filling this out, their signature is required.
- If applicable, provide details regarding any clerical errors to be reopened. Specify the original and corrected information.
- Clearly state the reason for disagreement with the original claim determination. This section allows you to specify your perspective.
- Attach all pertinent documentation that supports your request, ensuring your appeal is backed up with necessary evidence.
- Once all information is completed and documentation attached, review the form for accuracy and completeness.
- After finalizing the form, proceed to save changes, download, print, or share the form as needed for submission.
Take control of your healthcare claims. Complete your Medicare Reconsideration Form online today.
A redetermination must be requested in writing....Make a written request containing all of the following information: Beneficiary name. Medicare number. Specific service(s) and/or item(s) for which a redetermination is being requested. Specific date(s) of service. Name of the party, or the representative of the party.