Loading
Get Provider Claim Inquiry Form
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the Provider Claim Inquiry Form online
Filling out the Provider Claim Inquiry Form online is an essential step for providers looking to inquire about claims or request reconsiderations. This guide will help you understand each section of the form, ensuring that you complete it accurately and effectively.
Follow the steps to successfully complete the Provider Claim Inquiry Form.
- Click ‘Get Form’ button to obtain the form and open it in your online editor.
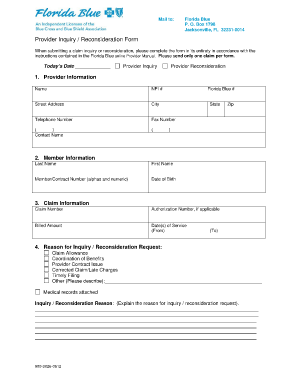
- In the 'Today’s Date' field, enter the current date to indicate when you are submitting the inquiry or reconsideration.
- In the 'Provider Information' section, fill in your name, NPI number, Florida Blue number, street address, city, telephone number, and fax number. Ensure all details are accurate for proper identification.
- Under 'Member Information', provide the member's last name, first name, member or contract number, and their date of birth. This information is critical for processing your inquiry.
- Complete the 'Claim Information' section by entering the claim number, authorization number if relevant, billed amount, and the date(s) of service. Include both the 'From' and 'To' dates for the service.
- In the 'Reason for Inquiry / Reconsideration Request' section, select the appropriate reason for your inquiry. If you choose 'Other', be sure to provide a description in the space provided.
- In the inquiry or reconsideration reason space, explain your reasons clearly and succinctly. You may attach additional medical records if necessary.
- Once you have filled out all sections of the form, review your entries for accuracy. After confirming that everything is correct, you can save changes, download, print, or share your completed form.
Start completing the Provider Claim Inquiry Form online now to ensure your claims are processed efficiently.
Related links form
WHAT IS A CORRECTED CLAIM? A corrected claim is a replacement of a previously billed claim that requires a revision to coding, service dates, billed amounts or member information. CORRECTED CLAIM BILLING REQUIREMENTS.
Industry-leading security and compliance
US Legal Forms protects your data by complying with industry-specific security standards.
-
In businnes since 199725+ years providing professional legal documents.
-
Accredited businessGuarantees that a business meets BBB accreditation standards in the US and Canada.
-
Secured by BraintreeValidated Level 1 PCI DSS compliant payment gateway that accepts most major credit and debit card brands from across the globe.