Loading
Get Cbiz Flex Benefits Claim Form
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the Cbiz Flex Benefits Claim Form online
Completing the Cbiz Flex Benefits Claim Form online is a straightforward process that enables users to submit their claims for reimbursement efficiently. This guide provides clear, step-by-step instructions to help you navigate the form with confidence.
Follow the steps to fill out the form correctly.
- Click ‘Get Form’ button to download the claim form and open it in your preferred online editor.
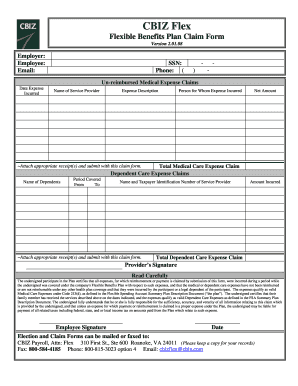
- Begin by entering your employer's name and your personal details, including your name, email address, Social Security number, and phone number.
- For un-reimbursed medical expense claims, fill in the date the expense was incurred, the name of the service provider, a brief description of the expense, the person for whom the expense was incurred, and the net amount. Be sure to attach appropriate receipts to substantiate these claims.
- Next, for any dependent care expense claims, provide the names of your dependents, the period covered (from what date to what date), and the name and Taxpayer Identification Number of the service provider. Again, ensure that you attach the necessary receipts.
- Sum up the total medical care expenses and the total dependent care expenses at the designated areas of the form.
- Review the declaration section before signing. This confirms that you understand the responsibility regarding the claims being submitted and that all expenses meet the program's requirements.
- Finally, sign and date the form, then save your changes. You can choose to print, download, or share the completed form as required.
Take the first step towards filing your claims online today!
Log in to the consumer portal at myplans.cbiz.com and select File a Claim under the Accounts link. Download the Mobile App through the AppStore or Google Play and search for “My Plans by CBIZ.”