Loading
Get Dd 2870
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the Dd 2870 online
The Dd 2870 is a vital form used for the authorization of disclosure of medical or dental information. This guide provides comprehensive, step-by-step instructions for filling out the form online to ensure a smooth and accurate submission.
Follow the steps to properly complete the Dd 2870 form online.
- Click the ‘Get Form’ button to obtain the Dd 2870 and open it in your preferred online document editor.
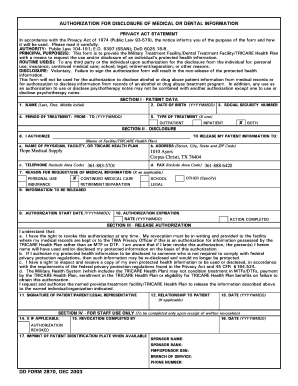
- In Section I, enter your patient data, including your name (last, first, and middle initial), date of birth in YYYYMMDD format, and social security number. Also, specify the period of treatment by entering the start and end dates in YYYYMMDD format.
- In section II, under the disclosure section, indicate to whom you are releasing your patient information by filling in the name of the physician, facility, or TRICARE Health Plan, along with their complete address and phone number. Include the reason for the request by marking the appropriate box for personal use, continued medical care, insurance, school, legal, retirement/separation, or other. If other, please specify.
- This section requires you to indicate what information will be released. Be specific about the medical records, reports, or information needed. Also, fill in the authorization start and expiration dates in YYYYMMDD format.
- In Section III, review the release authorization paragraph. By signing, you acknowledge that you understand your rights concerning the disclosure of your protected health information.
- Sign the form in the designated area, and if necessary, include your relationship to the patient if you are filling it out on their behalf. Lastly, date the form by entering the current date in YYYYMMDD format.
- Once you have completed the form, save any changes you made. You can then download, print, or share the Dd 2870 as needed for your records.
Start filling out your Dd 2870 online today to ensure timely processing of your medical information requests.
Authorization for Disclosure of Medical or Dental Information (DD Form 2870) Use this form to authorize an individual to release information that is protected under the Federal Privacy Act. This form is not valid to designate a representative for the Appeals process.