Loading
Get Universal Patient Authorization Form For Limited Disclosure Of Health Information - Palmsmg
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the UNIVERSAL PATIENT AUTHORIZATION FORM FOR LIMITED DISCLOSURE OF HEALTH INFORMATION - Palmsmg online
This guide provides a clear and supportive walkthrough for completing the Universal Patient Authorization Form for Limited Disclosure of Health Information. Medically relevant personal information should be shared with care, and this form allows you to control who can access your health details and for what purposes.
Follow the steps to fill out the form accurately and efficiently.
- Press the ‘Get Form’ button to access the Universal Patient Authorization Form and open it for editing.
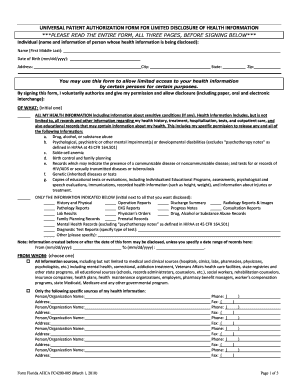
- Fill out the individual’s name and information section at the top of the form, including their date of birth, address, city, state, and zip code.
- In the section labeled 'OF WHAT,' choose to authorize the disclosure of either 'all my health information' or 'only the information indicated below.' Make the appropriate selection by placing your initials in the box beside your choice.
- If selecting specific information, initial next to each type of record you wish to disclose, such as history and physical, lab results, or mental health records.
- Indicate any specific date ranges for the records you wish to disclose, if applicable, by filling in the 'From' and 'To' dates.
- Select 'FROM WHOM' by choosing whether to authorize information from all sources or specific sources by indicating the name and address of the organizations or individuals.
- In the 'TO WHOM' section, list the persons or organizations that will receive your information by specifying their names and addresses.
- Check off all applicable purposes for the disclosure of the information, such as medical treatment, personal health records, or scientific research.
- Decide the effective period of your authorization by choosing either a specific date, a specific event, or the condition that it remains effective until it is withdrawn or upon your death.
- Sign and date the form at the bottom. If applicable, also provide the name and relationship to the patient for any legal representative.
- Once completed, review the form to ensure all information is accurate, then save your changes, and opt to download, print, or share the form as needed.
Complete your documents online with confidence and ensure your health information is disclosed accurately.
It is important to emphasize the difference between a use and a disclosure of PHI. In general, the use of PHI means communicating that information within the covered entity. ... Disclosure - The release, transfer, access to, or divulging of information in any other manner outside the entity holding the information.
Industry-leading security and compliance
US Legal Forms protects your data by complying with industry-specific security standards.
-
In businnes since 199725+ years providing professional legal documents.
-
Accredited businessGuarantees that a business meets BBB accreditation standards in the US and Canada.
-
Secured by BraintreeValidated Level 1 PCI DSS compliant payment gateway that accepts most major credit and debit card brands from across the globe.