Loading
Get Medical Record Release Form - Guthrie - Guthrie
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the Medical Record Release Form - Guthrie - Guthrie online
Filling out the Medical Record Release Form is an important step in managing your health information. This guide will walk you through each section of the form to ensure that you complete it accurately and efficiently.
Follow the steps to successfully complete the form.
- Click ‘Get Form’ button to obtain the form and open it in the editor.
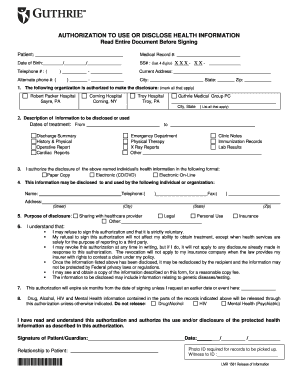
- Begin by completing your personal information at the top of the form. Fill in your full name, medical record number, date of birth, last four digits of your Social Security number, telephone number, current address, and an alternate phone number.
- In the section labeled 'The following organization is authorized to make the disclosure', check all the appropriate boxes that apply to your situation. This may include Robert Packer Hospital, Corning Hospital, Troy Hospital, and Guthrie Medical Group PC.
- For the 'Description of information to be disclosed or used' section, specify the relevant dates of treatment and check all that apply from the list of information categories provided. This may include discharge summaries, operative reports, lab results, and more.
- Indicate the format in which you would like to receive the disclosed information by selecting paper copy, electronic (CD/DVD), or electronic online.
- In the next section, provide the name, address, and telephone number of the individual or organization that will receive your health information.
- Specify the purpose of the disclosure by marking one or more of the options listed, such as sharing with a healthcare provider, for legal reasons, personal use, or insurance.
- Read the consent information regarding the voluntary nature of the authorization and the implications of disclosing your health information. Make sure you understand your rights.
- Fill in the expiration date of the authorization, which is typically six months from the date you sign unless you specify otherwise.
- Indicate whether you wish to exclude any specific types of sensitive information, such as drug/alcohol, HIV, or mental health records from being disclosed.
- Finally, sign and date the form. If you are a guardian or authorized representative, indicate your relationship to the patient.
- Once you have completed the form, you can save the changes, download a copy, print the form, or share it as needed.
Complete your Medical Record Release Form online today to manage your health information effectively.
How do I access my health records? Contact the custodian of your health records, such as a doctor, clinic or hospital, to request access. The custodian might ask you to make a formal request, in writing. You can write a letter or use this Request to Access Personal Health Information Form.
Industry-leading security and compliance
US Legal Forms protects your data by complying with industry-specific security standards.
-
In businnes since 199725+ years providing professional legal documents.
-
Accredited businessGuarantees that a business meets BBB accreditation standards in the US and Canada.
-
Secured by BraintreeValidated Level 1 PCI DSS compliant payment gateway that accepts most major credit and debit card brands from across the globe.