Loading
Get Attending Doctor ''s Request For Approval Of Variance And Carrier ''s Response State Of New York
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the attending doctor's request for approval of variance and carrier's response State of New York online
Filling out the attending doctor's request for approval of variance and carrier's response is essential for obtaining necessary medical treatment. This guide will provide a step-by-step process to help users understand each section of the form and complete it efficiently online.
Follow the steps to fill out the form accurately and effectively.
- Click ‘Get Form’ button to access the form and open it in the editor.
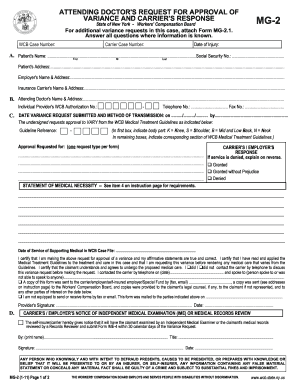
- Begin with the WCB case number and insurance carrier case number. Ensure these numbers are correctly entered as they are vital for processing.
- Fill in the date of injury, patient's name including first, middle initial, and last name, along with their social security number.
- Provide the patient's address, employer's name and address, and the insurance carrier's name and address to ensure they receive the request.
- Enter the attending doctor's name and address. Include their WCB authorization number and contact information such as telephone and fax numbers.
- Indicate the date of variance request submission and the method of transmission.
- State the guideline reference number clearly and specify the body part requiring variance by using the provided codes.
- In the statement of medical necessity section, provide a detailed explanation based on the requirements outlined in the instruction page.
- Certify that your statements are true and correct, and indicate whether you contacted the carrier before submitting the variance request.
- Submit the completed form and send it to the necessary parties including the workers' compensation board and the claimant’s legal counsel, if applicable.
- Finally, ensure to save changes, download, print, or share the completed form as required to finalize the process.
Ensure your variance requests are accurately submitted online for timely processing.
MG-2, ATTENDING DOCTOR'S REQUEST FOR APPROVAL OF VARIANCE AND INSURER'S RESPONSE This form requires the name and fax number or email address of the insurer's designated contact listed on the Workers' Compensation Board's website.
Industry-leading security and compliance
US Legal Forms protects your data by complying with industry-specific security standards.
-
In businnes since 199725+ years providing professional legal documents.
-
Accredited businessGuarantees that a business meets BBB accreditation standards in the US and Canada.
-
Secured by BraintreeValidated Level 1 PCI DSS compliant payment gateway that accepts most major credit and debit card brands from across the globe.