Loading
Get Nebraska Ownership/controlling Interest And ... - Dhhs Ne
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to use or fill out the NEBRASKA OWNERSHIP/CONTROLLING INTEREST AND CONVICTION DISCLOSURE online
Completing the Nebraska Ownership/Controlling Interest and Conviction Disclosure form is an essential step for entities aiming to engage with Nebraska Medicaid. This guide provides clear, step-by-step instructions to assist users in accurately filling out the form online.
Follow the steps to successfully complete the form.
- Use the 'Get Form' button to obtain the Nebraska Ownership/Controlling Interest and Conviction Disclosure form and open it in your editing tool.
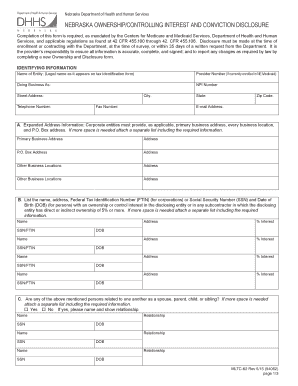
- Begin by filling in the identifying information. Include the legal name of the entity, provider number (if currently enrolled), doing business as name, NPI number, street address, city, state, zip code, telephone number, fax number, and email address.
- In section A, provide expanded address information. For corporate entities, list the primary business address, additional business locations, and any P.O. Box addresses. If you need more space, attach a separate list.
- In section B, list the names, addresses, Federal Tax Identification Numbers or Social Security Numbers, and dates of birth of individuals with an ownership or control interest in the disclosing entity. Attach additional sheets if necessary.
- Respond to section C's question regarding relationships. Indicate whether any of the above-mentioned individuals are related and, if so, specify their names and relationships.
- In section D, identify any managing employees within the disclosing entity by listing their names, Social Security Numbers, position titles, and dates of birth.
- Section E requires you to indicate if any person or entity with an ownership interest also has an ownership or controlling interest in any other Nebraska Medicaid provider. Provide the required names and interest percentages.
- In section F, list individuals who have ever been convicted of a criminal offense related to their involvement in Medicare, Medicaid, Waivers, CHIP, or Title XX services. Provide their names, dates of birth, and details of the convictions.
- Finally, complete the provider statement to certify that all information provided is true and accurate. Sign the form and include the printed name, title, and date.
- Once all sections are completed, ensure you save changes, then download, print, or share the form as necessary.
Start filling out your Nebraska Ownership/Controlling Interest and Conviction Disclosure form online today!
The Nebraska Medical Assistance Program, also known as the Medicaid Program, is a program that is jointly funded by the state and the Federal government to provide medical coverage to those who meet certain categorical eligibility criteria and who cannot afford to pay for medically necessary services.
Industry-leading security and compliance
US Legal Forms protects your data by complying with industry-specific security standards.
-
In businnes since 199725+ years providing professional legal documents.
-
Accredited businessGuarantees that a business meets BBB accreditation standards in the US and Canada.
-
Secured by BraintreeValidated Level 1 PCI DSS compliant payment gateway that accepts most major credit and debit card brands from across the globe.