Loading
Get Medical Necessity Review Form For Absorbent Products Mnr-ap - Mass
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the Medical Necessity Review Form For Absorbent Products MNR-AP - Mass online
Filling out the Medical Necessity Review Form for Absorbent Products is a crucial step in ensuring that users receive necessary medical supplies. This guide offers clear, step-by-step instructions to help you navigate the form effectively and understand its components.
Follow the steps to successfully complete the form.
- Press the ‘Get Form’ button to access the Medical Necessity Review Form. This will allow you to open and interact with the form conveniently.
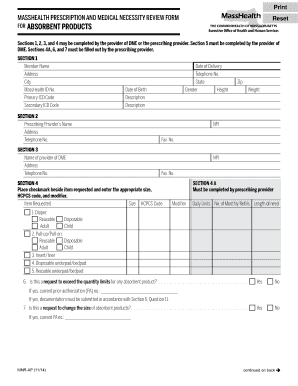
- In Section 1, fill out the member's name, address, city, MassHealth ID number, primary and secondary ICD codes, date of birth, gender, height, and weight. Ensure all details are accurate and up to date.
- Proceed to Section 2 and enter the prescribing provider’s name, address, telephone number, and NPI number. This information identifies who is prescribing the absorbent products.
- Fill in Section 3 with details of the provider of DME, including their name, address, telephone number, and NPI number.
- In Section 4, place a checkmark next to each item requested and enter the appropriate size, HCPCS code, and modifier. This indicates your specific needs and product types.
- For Section 4A, the prescribing provider must enter the daily units, the number of monthly refills, and the length of need for the product.
- Complete Section 6 by answering all applicable questions about the member's incontinence condition, prior treatments, and necessary documentation. Attach supporting clinical evidence as required.
- In Section 7, the prescribing provider must sign and date the form, certifying the accuracy of the information provided. The signature must be from an authorized individual, such as a physician, nurse practitioner, or physician assistant.
- Finally, you can save changes, download, print, or share the completed form as necessary. Ensure a copy is kept for records.
Complete the Medical Necessity Review Form online today to ensure timely access to needed absorbent products.
Related links form
Sample Format Letter of Medical Necessity Dear [Insert Contact Name]: [Insert Patient Name] has been under my care for [Insert Diagnosis] [Insert ICD-10-CM Code] since [Insert Date]. Treatment of [Insert Patient Name] with [medication] is medically appropriate and necessary and should be covered and reimbursed.
Industry-leading security and compliance
US Legal Forms protects your data by complying with industry-specific security standards.
-
In businnes since 199725+ years providing professional legal documents.
-
Accredited businessGuarantees that a business meets BBB accreditation standards in the US and Canada.
-
Secured by BraintreeValidated Level 1 PCI DSS compliant payment gateway that accepts most major credit and debit card brands from across the globe.