Loading
Get Dwc 09 Form
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the DWC 09 Form online
The DWC 09 Form is essential for reporting workplace injuries and documenting work status for employees seeking benefits. This guide provides comprehensive, step-by-step instructions to help you complete the form efficiently and accurately online.
Follow the steps to complete the DWC 09 Form online.
- Click ‘Get Form’ button to access the DWC 09 Form and open it in your preferred online editor.
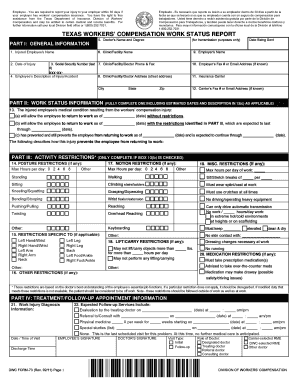
- Begin with Part I, where you will enter general information. Fill out sections for the injured employee's name, date of injury, and Social Security Number. Additionally, provide the doctor's name, clinic information, employer's name, and contact details.
- In Part II, complete the work status information. Indicate the medical condition's impact on the employee’s ability to return to work, including dates and any applicable restrictions.
- If applicable, complete Part III by detailing any activity restrictions. Specify posture, motion, lifting/carrying limits, and any medication restrictions.
- In Part IV, document treatment and follow-up appointments, including diagnosis information and expected services.
- Complete the form by obtaining signatures from the injured employee and the doctor, indicating the type of visit.
- After filling out the form, review all information for accuracy. You may then choose to save changes, download a copy, print the form, or share it as needed.
Complete your DWC 09 Form online today to ensure a smooth reporting process for your workplace injury.
Form DWC-85 is used to verify the independent relationship and the intent of the parties to exclude the independent contractor from the general contractor's workers' compensation insurance.