Loading
Get Employer ''s Initial Report Of Injury Wcb Claim No
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the Employer's Initial Report of Injury WCB Claim No online
Filling out the Employer's Initial Report of Injury WCB Claim No online is a critical step in reporting workplace injuries. This guide provides concise and supportive instructions to help you complete each section of the form with confidence.
Follow the steps to successfully complete the report online.
- Click ‘Get Form’ button to access the form and open it in your preferred PDF editor.
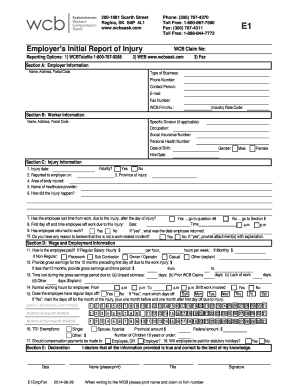
- Complete Section A: Employer Information by entering your organization's name, address, postal code, type of business, phone number, contact person, email, fax number, and WCB Firm No. Ensure all information is current and accurate.
- Fill out Section B: Worker Information by providing details about the injured worker, including specific division (if applicable), occupation, name, address, postal code, social insurance number, personal health number, date of birth, hire date, and gender.
- In Section C: Injury Information, record the injury date, date the incident was reported to the employer, area of the body injured, and name of the healthcare provider. Explain how the injury occurred and provide the province where the injury took place. Indicate if the injury resulted in a fatality and whether the worker lost time from work due to the injury.
- If the worker lost time from work, complete question #8 by recording the first day off and the time the employee left work due to the injury. Specify if the employee has returned to work and, if yes, the date of return. Also, clarify if you believe the incident is work-related.
- In Section D: Wage and Employment Information, describe how the employee is paid and provide gross earnings for the 12 months preceding the first day off due to the work injury. Document any time lost during this period due to unpaid sickness, prior WCB claims, or other reasons. Specify the normal working hours and regular days off.
- Finally, complete Section E: Declaration by providing your name, title, and the date. Ensure you sign the form to declare that all provided information is true and correct to the best of your knowledge.
- Once all sections are completed, you can save your changes, download the form, print it, or share it as needed.
Complete and submit your documents online to ensure a smooth claims process.
The employer is required to file an Employer's First Report of Injury or Illness [DWC FORM-001 Rev. 10/05] with the injured worker's insurance carrier, and the injured claimant or the claimant's representative within 8 days after the employee's absence from work or receipt of notice of occupational disease.
Industry-leading security and compliance
US Legal Forms protects your data by complying with industry-specific security standards.
-
In businnes since 199725+ years providing professional legal documents.
-
Accredited businessGuarantees that a business meets BBB accreditation standards in the US and Canada.
-
Secured by BraintreeValidated Level 1 PCI DSS compliant payment gateway that accepts most major credit and debit card brands from across the globe.