Loading
Get Ancillary Provider Network Participation Request Form - Health Net
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the Ancillary Provider Network Participation Request Form - Health Net online
This guide provides a comprehensive overview of how to complete the Ancillary Provider Network Participation Request Form for Health Net. By following the steps outlined, you will ensure that your application is filled out accurately and efficiently.
Follow the steps to complete the form online.
- Click ‘Get Form’ button to access the Ancillary Provider Network Participation Request Form and open it in your preferred online editor.
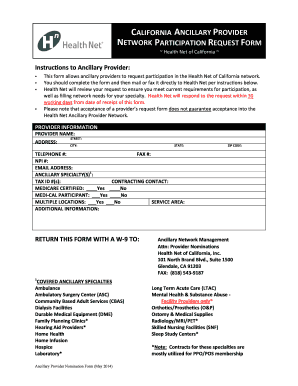
- Begin by filling in your provider information. Enter your full provider name, along with your address details including street, city, state, and zip code.
- Provide your contact details by entering your telephone number, fax number, NPI number, and email address in the respective fields.
- Specify your ancillary specialty or specialties. Be sure to list all relevant specialties to ensure an accurate representation of your services.
- Enter your tax identification numbers in the designated field.
- Indicate your contracting contact person, along with their contact details.
- Select whether you are Medicare certified and a Medi-Cal participant by checking the corresponding boxes.
- Indicate if you operate multiple locations and specify your service area to provide necessary context for your application.
- Use the additional information section to provide any other pertinent details that may support your request for network participation.
- Once all sections are filled out, save your changes and consider downloading or printing the completed form. Ensure to attach a W-9 form before submission.
- Submit your completed form by mailing or faxing it to the address provided: Ancillary Network Management, Attn: Provider Nominations, Health Net of California, Inc., 101 North Brand Blvd., Suite 1500, Glendale, CA 91203, or by faxing it to (818) 543-9187.
Complete your Ancillary Provider Network Participation Request Form online today to ensure your participation in the Health Net network.
Timely Filing of Claims When Health Net is the secondary payer, we will process claims received within 180 days after the later of the date of service and the date of the physician's receipt of an Explanation of Benefits (EOB) from the primary payer.
Industry-leading security and compliance
US Legal Forms protects your data by complying with industry-specific security standards.
-
In businnes since 199725+ years providing professional legal documents.
-
Accredited businessGuarantees that a business meets BBB accreditation standards in the US and Canada.
-
Secured by BraintreeValidated Level 1 PCI DSS compliant payment gateway that accepts most major credit and debit card brands from across the globe.