Loading
Get Delivery Report
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the Delivery Report online
Filling out the Delivery Report online is a straightforward process that ensures accurate documentation of services provided. This guide will walk you through each section of the form to help you complete it efficiently.
Follow the steps to complete the Delivery Report accurately.
- Click ‘Get Form’ button to obtain the Delivery Report and open it in the designated editor.
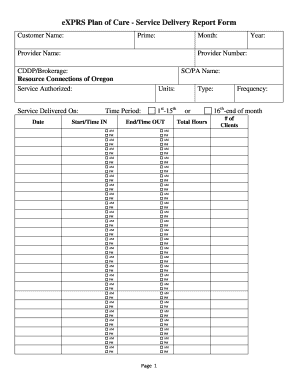
- Enter the customer name in the designated field. This should reflect the name of the recipient receiving the services.
- Fill in the 'Prime' field, indicating the primary service or program associated with the delivery of care.
- Provide the provider name and provider number. This information is essential for identifying the individual or organization delivering services.
- Specify the month and year for which the report is being submitted.
- Select the CDDP/Brokerage by entering 'Resource Connections of Oregon' or the relevant brokerage for your situation.
- Indicate the service authorized and the total units delivered, ensuring both figures align with the recipient’s service plan.
- Record the specific date the service was delivered, selecting either the 1st-15th or the 16th-end of the month as applicable.
- Fill in the start and end times using the AM/PM format, ensuring all relevant times are accurately recorded.
- Complete the service goal section to provide context about the aim of the activities performed.
- Use the progress notes section for any additional comments or observations. Attach extra pages if necessary.
- Sign the recipient/employer verification section, affirming the information reported is accurate and aligns with the service agreement.
- The provider/employee must sign their verification, confirming the data is truthful and does not exceed authorized limits.
- Initial the authorization for CDDP/Brokerage staff to enter the data into eXPRS for claims processing.
- After completing all fields and obtaining necessary signatures, submit the form to the CDDP or Brokerage that authorized the service.
Complete your Delivery Report online today to ensure prompt and accurate processing of your services.
A delivery receipt confirms delivery of your email message to the recipient's mailbox, but not that the recipient has seen it or read it. A read receipt confirms that your message was opened.
Industry-leading security and compliance
US Legal Forms protects your data by complying with industry-specific security standards.
-
In businnes since 199725+ years providing professional legal documents.
-
Accredited businessGuarantees that a business meets BBB accreditation standards in the US and Canada.
-
Secured by BraintreeValidated Level 1 PCI DSS compliant payment gateway that accepts most major credit and debit card brands from across the globe.