Loading
Get Aetna Nj Du31
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the Aetna Nj Du31 online
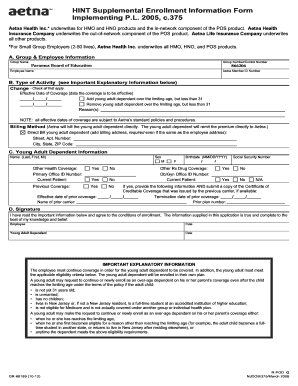
The Aetna Nj Du31 form is essential for managing supplemental enrollment for young adult dependents. This guide will assist you in filling out the form online efficiently and accurately, ensuring that you complete each section with the necessary information.
Follow the steps to complete the Aetna Nj Du31 form online.
- Press the ‘Get Form’ button to obtain the Aetna Nj Du31 form and open it for editing.
- In section A, provide the group name and group number/control number. For example, you can input 'Paramus Board of Education' and '866206'.
- Enter your name and Aetna member ID number in the respective fields in section A.
- In section B, check the type of activity you are reporting, such as changes to coverage or adding/removing a young adult dependent.
- Fill in the effective date of coverage in the designated space, ensuring the format is correct with month, day, and year.
- If applicable, indicate whether you are adding or removing a young adult dependent and provide reasons in the space provided.
- Specify the billing method for the young adult dependent. If you select 'Direct Bill,' include their billing address, even if it is the same as yours.
- Move to section C and enter the young adult dependent's name, birthdate, and sex. Input 'M' or 'F' as appropriate.
- Indicate if the young adult dependent has other health coverage and provide essential details, including the prior carrier and dates.
- In section D, confirm your agreement to the conditions by signing and dating the form.
- Once all sections are complete, review the information for accuracy. Save changes, download, print, or share the completed form as needed.
Complete your Aetna Nj Du31 form online today to ensure proper enrollment for your young adult dependent.
The length of your COBRA coverage continuation depends on the nature of the COBRA-qualifying event that entitled you to the coverage. For loss of coverage due to termination of em- ployment, reduction of hours, or leave of ab- sence, the employee and/or dependents are entitled to 18 months of COBRA coverage.