Loading
Get Cms-1513. Model Letter Announcing To Accredited Hospital After A Sample Validation Survey That The
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the CMS-1513. Model Letter Announcing To Accredited Hospital After A Sample Validation Survey online
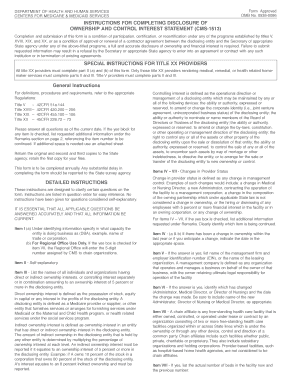
The CMS-1513 form is essential for disclosing ownership and control interest in healthcare facilities. Completing this form accurately ensures compliance with Medicare and Medicaid regulations and is crucial for maintaining contractual agreements and operational integrity.
Follow the steps to successfully complete the CMS-1513 form.
- Click ‘Get Form’ button to retrieve the CMS-1513 form and open it in an editable format.
- Begin with Section I, 'Identifying Information.' Provide the name of the entity, operating as, provider number, vendor number, contact information, and address of the facility.
- Proceed to Section II. Answer each yes or no question regarding ownership, criminal offenses, and managerial employment accurately. If any responses indicate 'yes', provide additional details in the remarks section on page 2.
- In Section III, list the names and addresses of individuals or organizations with a direct or indirect ownership interest of 5 percent or more. Include the type of entity and, if applicable, provide details on other Medicare/Medicaid facilities associated with the owners.
- Move on to Section IV. Indicate any changes in ownership or control from the past year and expectations for the near future. Clearly state the relevant dates of these changes.
- In Section V, specify if the facility is operated by a management company or leased partially or wholly. Enter any pertinent dates regarding changes in these operations.
- Section VI necessitates information about any changes in the Administrator, Director of Nursing, or Medical Director over the past year. If applicable, list any name changes.
- In Section VII, confirm if the facility is chain-affiliated and provide details about the corporation’s name, address, and EIN. If it was previously affiliated with a chain, ensure to include the necessary information.
- Lastly, Section VIII requests information about bed capacity changes within the past two years. State both current and prior bed counts and any years relevant to changes.
- Complete the form by typing the name of the authorized representative, providing their signature, title, and date. Finally, submit the form and retain a copy for your records.
Ensure compliance by completing the CMS-1513 form online today!
Related links form
These surveys are conducted to ascertain whether a provider/supplier meets applicable requirements for participation in the Medicare and/or Medicaid programs, and to evaluate performance and effectiveness in rendering a safe and acceptable quality of care.
Industry-leading security and compliance
US Legal Forms protects your data by complying with industry-specific security standards.
-
In businnes since 199725+ years providing professional legal documents.
-
Accredited businessGuarantees that a business meets BBB accreditation standards in the US and Canada.
-
Secured by BraintreeValidated Level 1 PCI DSS compliant payment gateway that accepts most major credit and debit card brands from across the globe.