Loading
Get Pdf: Worker Report Of Injury Form (c060) - January 2011. Wcb Worker Report Of Injury Form (c060)
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the PDF: Worker Report Of Injury Form (C060) - January 2011 online
Filling out the Worker Report of Injury Form (C060) is an essential step for individuals who have experienced an injury or occupational disease. This guide provides straightforward instructions to help you complete the form accurately and efficiently, ensuring your report is submitted correctly.
Follow the steps to fill out the form successfully.
- Click 'Get Form' button to obtain the form and open it in your preferred PDF editor.
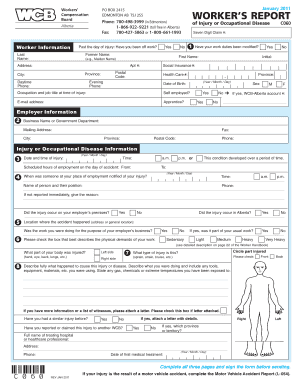
- Provide your worker information: Fill in your last name, first name, and former name if applicable. Include your address, daytime phone number, social insurance number, postal code, province, and date of birth.
- Indicate if you have been off work since the day of your injury and if your work duties have been modified. Include your employment status, such as self-employed or apprentice.
- Complete the employer information section: Provide the business name or government department name, mailing address, phone number, and fax information.
- Fill in the injury or occupational disease information. Enter the date and time of your injury, scheduled hours of employment, location of the accident, and notify whether it was reported immediately.
- Describe the injury: Include the part of the body injured, type of injury sustained, and provide a detailed account of the incident, including any tools or materials used.
- Complete the time lost/return to work information by providing dates, if you missed work and whether your employer will pay you during this time.
- Fill out the wage information, indicating your rate of pay at the time of the accident and any additional taxable benefits received.
- In the declaration and consent section, read the statement carefully. Print your name, sign, and date to confirm the information provided is accurate.
- Once all sections are completed, review the document for accuracy. You can then save changes, download, print, or share the completed form as needed.
Get started on your Worker Report of Injury Form online to ensure your claim is processed without delay.
The Employer's First Report of Injury or Illness provides information on the claimant, employer, insurance carrier and medical practitioner necessary to begin the claims process. Details of the claimant's employment and circumstances surrounding the injury or illness are also requested.
Industry-leading security and compliance
US Legal Forms protects your data by complying with industry-specific security standards.
-
In businnes since 199725+ years providing professional legal documents.
-
Accredited businessGuarantees that a business meets BBB accreditation standards in the US and Canada.
-
Secured by BraintreeValidated Level 1 PCI DSS compliant payment gateway that accepts most major credit and debit card brands from across the globe.