Loading
Get Provider Service Requisition Form - Uhccommunityplan.com
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the Provider Service Requisition Form - UHCCommunityPlan.com online
Filling out the Provider Service Requisition Form is essential for obtaining services for enrolled members. This guide provides a step-by-step approach to help you complete the form accurately and efficiently online.
Follow the steps to successfully fill out the Provider Service Requisition Form.
- Press the 'Get Form' button to access the Provider Service Requisition Form and open it in your preferred online editor.
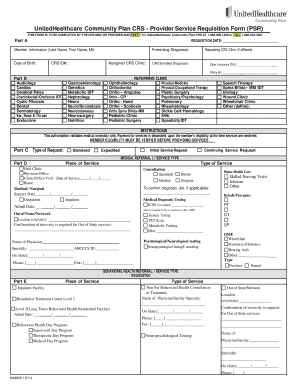
- In Part A, enter the requisition date, the member's last name, first name, middle initial, date of birth, CRS ID number, and the assigned CRS clinic's name. If applicable, also fill in the requesting CRS clinic's name and the member's presenting diagnosis.
- Still in Part A, identify any other insurance by providing the name of the insurance company and the corresponding policy numbers.
- In Part B, select the referring clinic specialty that corresponds to the service being requested. If the specialty is not listed, choose 'Other' and define the specialty.
- Move to Part C, where you will choose the type of request. Indicate whether the request is standard or expedited, and specify if it is the initial service or a continuing service request.
- In Part D, select the place of service where the procedure will occur and enter relevant dates like office visit date or surgery date as required. Include the city and state if out-of-state services are necessary.
- Continue in Part D by selecting the type of service requested. Provide additional information on medical diagnostic tests if relevant.
- In Part E, specify the type of behavioral health service requested and complete the information regarding the service's place of performance.
- Part F requires you to indicate whether the referral was made following a visit at the CRS Clinic or a physician's office. Include the name, specialty, and contact information of the physician.
- Complete Part G and Part H with the servicing provider's information, including their name, address, tax ID number, and AHCCCS ID if applicable.
- Lastly, in Part I, describe the requested service, enter the related CPT/HCPCS codes, number of units, service frequency, dates of service, and the reason for the service.
- Once you have filled in all required sections accurately, you can now save your changes, download, print, or share the completed form as necessary.
Complete your documents online with ease and ensure all information is filled out accurately.
Our Member Services is available to answer your questions and help you get the care you need. Just call us at 1-800-414-9025. We can help you between 8 a.m. and 5 p.m. Monday, Tuesday, Thursday, and Friday and 8 a.m. to 8 p.m. on Wednesday.
Industry-leading security and compliance
US Legal Forms protects your data by complying with industry-specific security standards.
-
In businnes since 199725+ years providing professional legal documents.
-
Accredited businessGuarantees that a business meets BBB accreditation standards in the US and Canada.
-
Secured by BraintreeValidated Level 1 PCI DSS compliant payment gateway that accepts most major credit and debit card brands from across the globe.