Loading
Get Prior Authorization Request Form - Sfhp
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to use or fill out the Prior Authorization Request Form - Sfhp online
Filling out the Prior Authorization Request Form for Sfhp can seem daunting, but understanding each component will help streamline the process. This guide provides you with comprehensive, step-by-step instructions to ensure that your request is completed accurately and efficiently, facilitating a smooth online experience.
Follow the steps to fill out the Prior Authorization Request Form accurately.
- Press the ‘Get Form’ button to obtain the Prior Authorization Request Form, which you can then open in the designated online format.
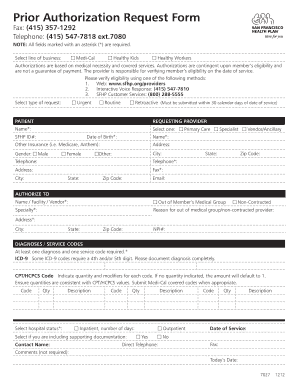
- Fill out the required fields marked with an asterisk (*). Start by selecting the line of business that applies to the patient: Medi-Cal, Healthy Kids, or Healthy Workers.
- Indicate the type of request you are submitting. You can choose from Urgent, Routine, or Retroactive, ensuring that you understand the conditions associated with each option.
- In the 'Patient' section, enter the patient's name, SFHP ID number, date of birth, gender, city, state, telephone number, and address. Be sure to confirm your selection under gender.
- Move to the 'Requesting Provider' section to input your name, type of provider (e.g., Primary Care, Specialist, Vendor/Ancillary), telephone, and email address.
- In the 'Authorize To' section, fill in the details for the name, facility, or vendor seeking authorization. Select the specialty and fill in the address details, including city, state, and zip code.
- Enter the NPI number of the provider to ensure proper processing.
- Proceed to the 'Diagnoses / Service Codes' section. You must provide at least one diagnosis and one service code. Make sure to document ICD-9 codes completely and indicate any required modifiers.
- Select the appropriate hospital status (inpatient or outpatient) and provide the number of inpatient days if applicable.
- Check the box if you are including supporting documentation and fill in the contact name and direct telephone number for follow-up.
- Provide the date of service, and feel free to add any comments in the optional comment section.
- Finally, save your completed form, and use the options available to download, print, or share the form as needed.
Complete your Prior Authorization Request Form online today to ensure timely processing and approvals.
Related links form
Free Printable Medical Forms Blood Pressure Health Check Log
Generalitat De Catalunya Departament D Ensenyament Serveis Territorials 1 / 1 G409-006/02-11 Sol
Chapter 22 Quizzes And Test.pdf - Esperanza-US History Summer ...
ID - Financial - Schedule For Legal Relating To Payments From Gay Homsey To Hacking Sheet 1 And
Call us today at 1-888-4LA-CARE (1-888-452-2273) to apply for health care coverage. L.A. Care Health Plan representatives are available 24 hours a day, 7 days a week, including holidays to help you.