Loading
Get Cms 1500 Submission Sample - Wellcare
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the CMS 1500 Submission Sample - WellCare online
Filling out the CMS 1500 Submission Sample - WellCare form is essential for efficiently processing your healthcare claims. This guide provides a clear, step-by-step approach to ensure accurate completion of this critical document.
Follow the steps to complete the CMS 1500 Submission Sample effectively.
- Press the ‘Get Form’ button to obtain the CMS 1500 Submission Sample and open it for editing.
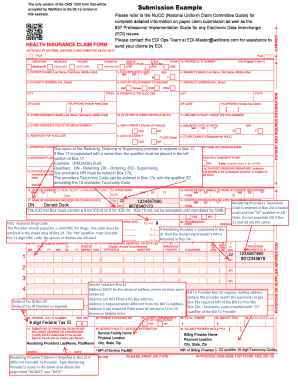
- In Box 17, enter the name of the referring, ordering, or supervising provider. If you fill this box, include the appropriate qualifier in the left section, using 'DN' for referring, 'DK' for ordering, or 'DQ' for supervising.
- Input the provider's NPI in Box 17b. Optionally, provide the Taxonomy Code in Box 17a, preceded by the qualifier 'ZZ'.
- In the ICD Ind Box, indicate '9' for ICD-9 or '0' for ICD-10, noting that ICD-10 will not be accepted until mandated by CMS.
- For any drugs, list a valid NDC in the shaded area of Box 24, starting with the 'N4' qualifier. Ensure there are no spaces or dashes in the 11 digit code.
- Enter the rendering provider's Taxonomy Code in Box 24J, along with the 'ZZ' qualifier in Box 24I. Do not populate Box 24J if Boxes 31 and 33 are the same.
- If the Rendering Provider is identified in Box 31, provide the NPI in Box 24J.
- Fill out Box 25 with the required Federal Tax ID Number.
- In Box 32, enter the physical address where services were rendered. Note that this address cannot be a PO Box and is necessary if different from the Bill To Address.
- Provide the mailing address in Box 33, as well as the NPI in Box 33a. Add the Taxonomy code with the 'ZZ' qualifier in Box 33b.
- If the Rendering Provider's name differs from the Bill To Provider, type their name in the designated blank area above the 'SIGNED' and 'DATE' fields.
- Review all entries for accuracy and completeness. Save your changes, download, print, or share the form as needed.
Complete your forms online efficiently and ensure swift claims processing!
Only uppercase characters should be used for procedure codes and modifiers. This is a required field. Enter the diagnosis code reference number or letter (as appropriate, per form version) as shown in Item 21 to relate the date of service and the items or services rendered to the primary diagnosis.