Loading
Get Gp45888-12 Get.doc. Health Benefits Claim Form To Be Completed By The Insured Member For Use With
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the GP45888-12 Get.doc. Health Benefits Claim Form To Be Completed By The Insured Member For Use With online
This guide provides a clear and comprehensive overview of how to accurately complete the GP45888-12 Get.doc. Health Benefits Claim Form. By following these instructions, users can ensure that they submit the necessary information for processing their health benefits claims efficiently.
Follow the steps to complete your health benefits claim form online.
- Click ‘Get Form’ button to obtain the form and open it in the editor.
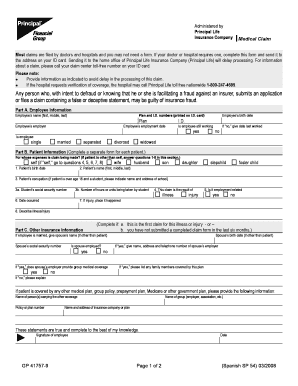
- Begin filling out Part A, Employee Information. Include the employee's full name, plan and ID numbers, employee's birth date, employment date, current employment status, and marital status.
- Proceed to Part B, Patient Information. Indicate if the claim is for the insured person or another individual, and complete the information including the patient's birth date, full name, and occupation.
- In Part C, Other Insurance Information, provide details about any other insurance plans covering the patient. Include the spouse's information if applicable.
- Complete Part D, Authorization for Release of Information. Ensure the employee and patient (if applicable) sign and date the authorization.
- Attach any required supporting documents, such as itemized bills or additional forms.
- Review all information for accuracy and completeness before submission.
- Once finalized, users can save the changes, download, print, or share the completed form as needed.
Complete your health benefits claim form online to ensure timely processing.
The CMS-1500 form is the standard claim form used by a non-institutional provider or supplier to bill Medicare carriers and durable medical equipment regional carriers (DMERCs) when a provider qualifies for a waiver from the Administrative Simplification Compliance Act (ASCA) requirement for electronic submission of ...
Industry-leading security and compliance
US Legal Forms protects your data by complying with industry-specific security standards.
-
In businnes since 199725+ years providing professional legal documents.
-
Accredited businessGuarantees that a business meets BBB accreditation standards in the US and Canada.
-
Secured by BraintreeValidated Level 1 PCI DSS compliant payment gateway that accepts most major credit and debit card brands from across the globe.