Loading
Get Termination Form - Best Life
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the Termination Form - Best Life online
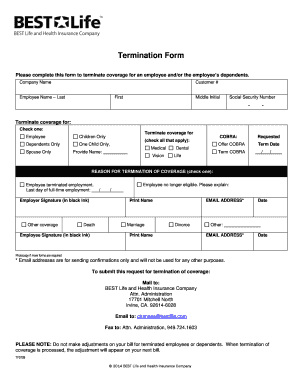
This guide will assist you in completing the Termination Form for Best Life. By following these steps, you will ensure that you accurately provide all necessary information to terminate coverage for the employee and/or their dependents.
Follow the steps to ensure accurate completion of the form.
- Click ‘Get Form’ button to obtain the form and open it in your preferred editor.
- Begin by entering the company name in the designated field.
- Input the customer number in the corresponding section to identify the account.
- Fill in the employee's name, including last name, first name, and middle initial as applicable.
- Provide the social security number in the specified format (XXX-XX-XXXX).
- Select the appropriate option to indicate who the coverage termination is for by checking one of the provided boxes: Employee, Children Only, Dependents Only, One Child Only, Spouse Only.
- If COBRA applies, check all relevant boxes for the coverage types: Medical, Vision, Dental, Life, and indicate if COBRA is being requested. Be sure to provide the name where required.
- Enter the requested termination date in the format MM/DD/YYYY.
- Indicate the reason for termination of coverage by checking the appropriate box and providing additional details if necessary.
- Obtain the required signatures. The employer must sign in black ink, followed by printing their name and date. The employee must also sign in black ink, print their name and date.
- If additional forms are required, make a photocopy of the completed form for your records.
- Once all sections are filled out, you can choose to save changes, download, print, or share the completed form as needed.
Complete your Termination Form online to manage employee coverage efficiently.
Loss of Coverage Letter – Letter from your previous health carrier indicating an involuntary loss of coverage. The supporting document must indicate your name, the names of any dependents that were covered under the prior plan and the date the previous health coverage ended.