Loading
Get Mirixapro
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the Mirixapro online
Filling out the Mirixapro authorization form online is a straightforward process, designed to enable pharmacies to designate authorized users efficiently. This guide provides detailed instructions on completing each section of the form to ensure accuracy and compliance.
Follow the steps to complete the Mirixapro form online.
- Click the ‘Get Form’ button to obtain the form and open it in your preferred document editor.
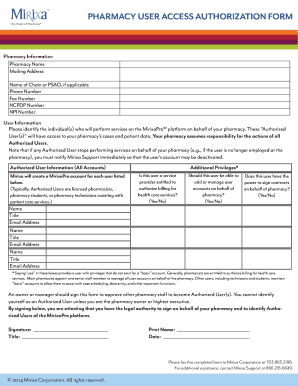
- Begin by entering the pharmacy information. Fill in the pharmacy name, mailing address, and include details such as the phone number, fax number, NCPDP number, and NPI number if applicable.
- Identify the authorized users. In this section, list the individuals who will be performing services on the MirixaPro platform. Ensure to include names, titles, and email addresses for each user.
- For each authorized user, indicate whether they are licensed pharmacists, pharmacy students, or pharmacy technicians assisting with patient care services by selecting the appropriate options.
- Address the additional privileges. Respond to the questions regarding whether the user is entitled to authorize billing or manage user accounts by selecting 'Yes' or 'No' for each field.
- Obtain the required signature. An owner or manager should sign the form to approve the designation of authorized users. Ensure that the individual signing has the legal authority to do so.
- Complete the signature block with the individual's title, printed name, and date of signing.
- Once the form is fully completed, you may save your changes, download the document, or print it for submission. You will need to fax the completed form to Mirixa Corporation at 703.865.2198.
Take the next step and complete your Mirixapro authorization form online today!
In order to qualify for the MTM program, you must meet all three of the following criteria: Have three of the five following conditions: 2020 conditions: Chronic Heart Failure (CHF), Rheumatoid Arthritis, Diabetes, Dyslipidemia (Abnormal Cholesterol), or Asthma, AND.