Loading
Get Partnership Raf Form
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the Partnership Raf Form online
This guide provides a clear, step-by-step process for users to complete the Partnership Raf Form online. It is designed to help you navigate each section of the form effectively, ensuring that you provide accurate and complete information.
Follow the steps to successfully complete the Partnership Raf Form.
- Press the ‘Get Form’ button to acquire the Partnership Raf Form and open it in your preferred digital editor.
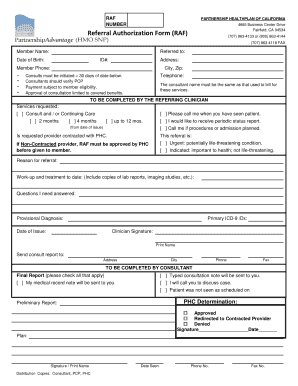
- Begin filling out the form by entering the member’s name in the designated field. Make sure the name matches the official documents for verification purposes.
- Provide the member's date of birth in the specified format. This information is crucial for identity verification.
- Enter the member's ID number as shown on their health plan documents to ensure correct processing.
- Fill in the member's address, including city and zip code. Accurate information will aid in communication and follow-up.
- Record the member's phone number, ensuring it is current and reachable for any necessary follow-ups.
- Indicate the services requested by selecting the appropriate boxes, such as 'Consult and/or Continuing Care.'
- Document the reason for referral and any relevant medical history, including copies of lab reports and imaging studies.
- Complete the clinician signature and print name fields, affirming that all information provided is true and accurate.
- Finalize the form by reviewing all entries for accuracy. Save your changes before downloading, printing, or sharing the form as needed.
Complete your Partnership Raf Form online today to streamline your referral process.
Partnership HealthPlan of California is a non-profit community based health care organization that contracts with the State to administer Medi-Cal benefits through local care providers to ensure Medi-Cal recipients have access to high-quality comprehensive cost-effective health care.