Loading
Get Unitedhealthcare Claim Submission / Withdrawal Request Form
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the UnitedHealthcare Claim Submission / Withdrawal Request Form online
This guide provides clear, step-by-step instructions on how to complete the UnitedHealthcare Claim Submission / Withdrawal Request Form online. Follow these instructions carefully to ensure a smooth and efficient claim submission process.
Follow the steps to complete your claim submission form online.
- Press the ‘Get Form’ button to access the UnitedHealthcare Claim Submission / Withdrawal Request Form and open it for editing.
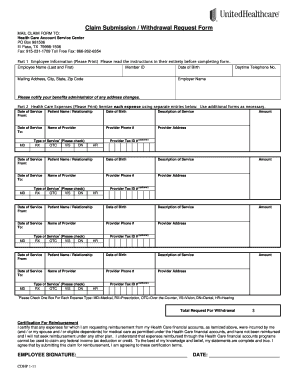
- Begin with Part 1 of the form. Fill in all required fields such as your name, Member ID, date of birth, mailing address, daytime telephone number, and employer name. Ensure this information is clear and legible.
- Proceed to Part 2 for Health Care Expenses. List each expense by itemizing them clearly. Use separate entries for each service by including the date of service, patient name and relationship, description of the service, provider name, phone number, and address.
- Indicate the type of service for each expense in the provided checkboxes. Options include Medical, Prescription, Over-the-Counter, Vision, Dental, and Hearing.
- Include the total requested amount at the bottom of Part 2. Ensure the total reflects all itemized expenses accurately.
- Read and complete the Certification for Reimbursement section. Sign and date the form to affirm that the expenses listed are valid and have not been previously reimbursed.
- Before submission, make copies of the completed form and all documentation for your personal records. Attach itemized receipts and ensure they meet the specified requirements.
- Finally, mail or fax the completed form and all necessary documentation to the Health Care Account Service Center at the address or fax number provided on the form. Ensure that your reimbursement request is postmarked before your plan's filing deadline.
Complete your UnitedHealthcare Claim Submission / Withdrawal Request Form online today for swift processing of your claims.
The other way to claim your health insurance is via reimbursement. You can pay for the medical expenses upfront and get the treatment done, and later submit all the bills to your insurer. Upon assessment of the bills, the insurer reimburses the expenses that you have incurred based on your sum assured limit.
Industry-leading security and compliance
US Legal Forms protects your data by complying with industry-specific security standards.
-
In businnes since 199725+ years providing professional legal documents.
-
Accredited businessGuarantees that a business meets BBB accreditation standards in the US and Canada.
-
Secured by BraintreeValidated Level 1 PCI DSS compliant payment gateway that accepts most major credit and debit card brands from across the globe.