Loading
Get Subscribers Statement Of Claim
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the Subscribers Statement Of Claim online
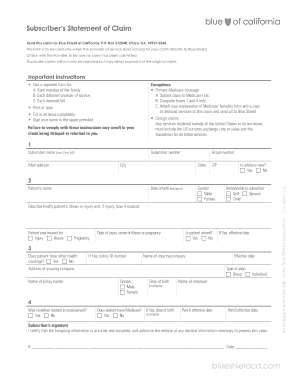
The Subscribers Statement Of Claim is an essential document for individuals seeking reimbursement from Blue Shield of California when their service provider has not submitted a claim directly. This guide provides clear, step-by-step instructions to help users complete this form accurately and efficiently.
Follow the steps to successfully fill out the Subscribers Statement Of Claim.
- Click the ‘Get Form’ button to access the Subscribers Statement Of Claim. This will allow you to obtain the document in a suitable format for filling out online.
- Begin by entering your subscriber name in the designated section, including your last name, first name, and middle initial. Make sure this information matches the records held by Blue Shield.
- Provide your subscriber number on the next line. This number is crucial for identifying your account with Blue Shield.
- Complete your mailing address, including street, city, state, and ZIP code. Indicate if your address has changed using the 'Is address new?' option.
- Enter your date of birth using the format month/day/year. Select your gender by checking the appropriate box.
- Indicate your relationship to the subscriber by selecting either 'Self', 'Spouse', or 'Child'.
- Briefly describe the patient’s illness or injury, including details about how the injury occurred, if applicable.
- Choose the appropriate box to indicate whether the patient was treated for an injury, illness, or pregnancy. Enter the date related to the injury, illness onset, or pregnancy.
- Answer whether the patient is retired and, if applicable, provide the effective date.
- Indicate if the patient has other health coverage. If yes, fill in the policy ID number and the name and address of the insuring company.
- Complete details such as the name of the policyholder, type of plan (group or individual), gender, date of birth, and employer’s name.
- State whether the condition was related to employment. Also, indicate if the patient has Medicare and provide relevant effective dates if applicable.
- Sign your name in the designated space, certifying that the information is accurate and complete, and include the date of signing.
- Once all fields are completed, save the document for your records. You may also download, print, or share the completed form as needed.
Complete your Subscribers Statement Of Claim online to ensure smooth processing of your claim.
Get form
Experience a faster way to fill out and sign forms on the web. Access the most extensive library of templates available.
How to fill out a CMS-1500 form The type of insurance and the insured's ID number. The patient's full name. The patient's date of birth. The insured's full name, if applicable. The patient's address. The patient's relationship to the insured, if applicable. The insured's address, if applicable. Field reserved for NUCC use.
Get This Form Now!
Use professional pre-built templates to fill in and sign documents online faster. Get access to thousands of forms.