Loading
Get Wellcare Medicare Coverage Determination Request Form
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the WellCare Medicare Coverage Determination Request Form online
Filling out the WellCare Medicare Coverage Determination Request Form is an important step for users seeking coverage for specific medications. By following this comprehensive guide, you will gain an understanding of each section of the form and how to complete it efficiently online.
Follow the steps to complete your coverage determination request form online.
- Press the ‘Get Form’ button to access the WellCare Medicare Coverage Determination Request Form. This will allow you to open the form in a suitable editor.
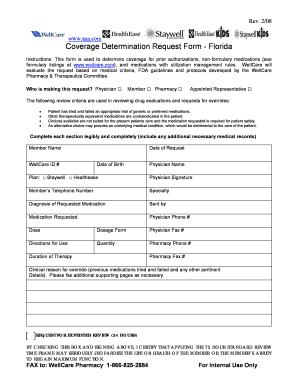
- Begin the form by indicating who is making the request. Select one of the options: Physician, Member, Pharmacy, or Appointed Representative by marking the appropriate box.
- Fill out the member's information. This includes the Member Name, WellCare ID Number, Date of Request, Date of Birth, and Member's Telephone Number. Ensure that these fields are completed legibly.
- Provide the Physician's details. Enter the Physician Name, Specialty, and their contact information, including Physician Phone Number and Physician Fax Number.
- Complete the medication details. Specify the Medication Requested, Dose, Dosage Form, Directions for Use, and the Quantity required.
- State the Duration of Therapy and include any additional clinical details relevant to your request in the Clinical reason for override section, such as previous medications tried and failed.
- If expedited review is necessary, check the box indicating that the standard 72-hour review timeframe may jeopardize the health of the member. Remember to sign here as well.
- Once all sections are thoroughly filled out, review the form for accuracy. You can then save changes, download, print, or share the form as needed.
Complete your WellCare Medicare Coverage Determination Request Form online today to ensure timely processing.
WellCare: 1-888-453-2534. TTY: 1-877-247-6272.