Loading
Get Wellcare Injectable Infusion Form
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the Wellcare Injectable Infusion Form online
Filling out the Wellcare Injectable Infusion Form online is an essential process for obtaining the necessary medical authorization. This guide will provide you with detailed steps to ensure that you complete the form accurately and efficiently.
Follow the steps to correctly fill out the form
- Click ‘Get Form’ button to access the form and open it in your preferred viewer.
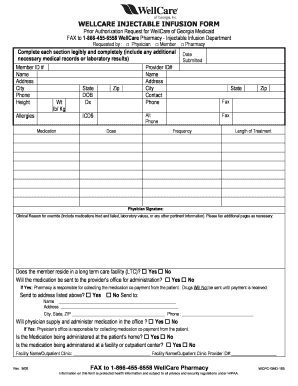
- Begin by entering the member ID number, which is critical for processing the request.
- Fill in the member's personal information, including their full name, address, city, and phone number.
- Record the member's height and weight, indicating pounds or kilograms as appropriate.
- Document any known allergies the member may have, which is important for medication safety.
- Input the member's date of birth (DOB) and the relevant diagnosis (Dx).
- Provide the healthcare provider's information, including their ID number, name, address, city, and contact phone number.
- Specify the medication details, including dosage, frequency, length of treatment, and corresponding ICD9 codes.
- Ensure the clinical reason for the override is clearly articulated, along with any pertinent medical records or laboratory results.
- Indicate if the member resides in a long-term care facility and whether the medication will be sent to the provider’s office for administration.
- Provide the name and address if the medication needs to be sent elsewhere.
- State whether the physician will supply and administer the medication in their office.
- Determine if the medication will be administered at the patient’s home or at a facility/outpatient center, and fill in the relevant facility details.
- Once you complete all sections, you may save your changes, download the form, print it, or share it as needed.
Complete your Wellcare Injectable Infusion Form online today for quick processing!
Wellcare Prescription Drug Plans: 1-866-859-9084 (TTY 711) Monday–Friday, 8 a.m. to 8 p.m.
Industry-leading security and compliance
US Legal Forms protects your data by complying with industry-specific security standards.
-
In businnes since 199725+ years providing professional legal documents.
-
Accredited businessGuarantees that a business meets BBB accreditation standards in the US and Canada.
-
Secured by BraintreeValidated Level 1 PCI DSS compliant payment gateway that accepts most major credit and debit card brands from across the globe.