Loading
Get Wellcare Injectable Infusion Form
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the Wellcare Injectable Infusion Form online
This guide will provide you with clear, step-by-step instructions on how to properly complete the Wellcare Injectable Infusion Form online. Following these steps will ensure that your submission is accurate and complete.
Follow the steps to fill out the Wellcare Injectable Infusion Form carefully.
- Click ‘Get Form’ button to obtain the form and open it in the online editor.
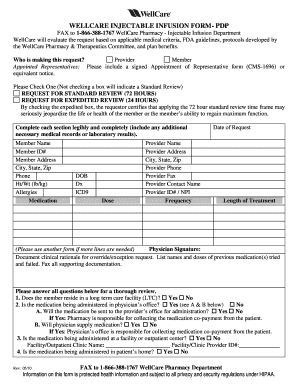
- Identify who is making the request by selecting the appropriate option: provider, member, or appointed representative. If you are an appointed representative, ensure you include a signed Appointment of Representative form (CMS-1696) or an equivalent notice.
- Choose between requesting a standard review or an expedited review. Check the box associated with your choice. Remember, not checking a box defaults to a standard review.
- Fill out the member's information completely. This includes the member's name, member ID, address, city, state, zip, phone number, height, weight, allergies, and current medication.
- Provide the member's date of birth, diagnosis, ICD-9 code, dosage, and any relevant provider details such as name, address, phone, fax, contact name, and provider ID/NPI.
- Specify the frequency of the medication and the date of request as well as the expected length of treatment. If additional lines are needed, use another form.
- The physician must sign the document, and you should provide clinical rationale for any override or exception requests. List names and doses of previous medications tried and failed.
- Answer the questions regarding the member's living situation: long-term care facility, physician's office administration, facility/outpatient clinic, or at-home administration. Fill in any required details where necessary.
- After filling out the form, review all information for accuracy and completeness. Ensure any required supporting documentation is attached.
- Save changes, and then download, print, or share the completed form as needed. FAX the form to 1-866-388-1767 WellCare Pharmacy Department.
Start your document filing process by completing the Wellcare Injectable Infusion Form online today.
Wellcare Prescription Drug Plans: 1-866-859-9084 (TTY 711) Monday–Friday, 8 a.m. to 8 p.m.
Industry-leading security and compliance
US Legal Forms protects your data by complying with industry-specific security standards.
-
In businnes since 199725+ years providing professional legal documents.
-
Accredited businessGuarantees that a business meets BBB accreditation standards in the US and Canada.
-
Secured by BraintreeValidated Level 1 PCI DSS compliant payment gateway that accepts most major credit and debit card brands from across the globe.