Loading
Get Authorization To Use And/or Disclosure Protected Health Information (10/27/11).pdf
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to use or fill out the Authorization To Use And/or Disclosure Protected Health Information (10/27/11).pdf online
This guide provides a clear and user-friendly approach to completing the Authorization To Use And/or Disclosure Protected Health Information form, ensuring you can fill it out accurately online. Follow these steps to navigate the form effectively and understand what each section requires.
Follow the steps to successfully complete the form online.
- Click the ‘Get Form’ button to access the Authorization To Use And/or Disclosure Protected Health Information (10/27/11) form and open it in your preferred editor.
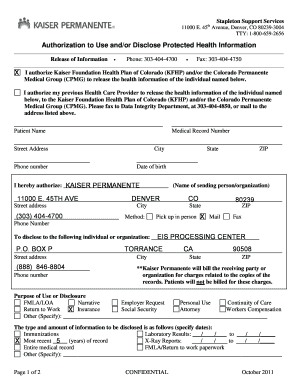
- Start by filling in the patient name in the designated field. This should be the full legal name of the individual whose health information is being disclosed.
- Next, provide the medical record number for the patient, if known. This helps the healthcare provider to identify the specific records.
- Complete the street address, city, state, and ZIP code fields for the patient. This information is crucial for correspondence.
- Fill in the phone number and date of birth of the patient to further verify identity and for contact purposes.
- In the section titled 'I hereby authorize,' specify the name of the organization or person sending the information. For instance, you may enter 'Kaiser Permanente'.
- Indicate the method by which the information will be disclosed: choose between pick up in person, mail, or fax by marking the appropriate box.
- Complete the fields for the individual or organization that will receive the disclosed information. Ensure you include the full address and phone number.
- Select the purpose of use or disclosure from the options provided, detailing if it’s for FMLA, insurance, or other specified reasons. You may also include any other purposes by writing them in the provided space.
- Specify the type and amount of information to be disclosed, including any relevant time periods, such as for immunizations or lab results.
- Indicate the format in which you would like to receive the records, either paper format or electronic copies.
- Sign and date the form at the bottom. If you are signing as a representative, include your name and relationship, along with any necessary legal documentation.
- Review all sections for accuracy and completeness before saving your changes, downloading the form, or printing it out for submission.
Complete your document online today to manage your health information effectively.
A covered entity may disclose PHI for its own payment activities or the payment activities of a healthcare provider or another covered entity without authorization by the patient or his/her personal representative. ... Covered entities are not currently required to account for payment disclosures.
Industry-leading security and compliance
US Legal Forms protects your data by complying with industry-specific security standards.
-
In businnes since 199725+ years providing professional legal documents.
-
Accredited businessGuarantees that a business meets BBB accreditation standards in the US and Canada.
-
Secured by BraintreeValidated Level 1 PCI DSS compliant payment gateway that accepts most major credit and debit card brands from across the globe.