Loading
Get Employer Provider Network Inc
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the Employer Provider Network Inc online
Filling out the Employer Provider Network Inc contract request form online can appear complex, but with clear guidance, the process becomes manageable. This guide offers step-by-step instructions to ensure you complete the form accurately and efficiently.
Follow the steps to successfully complete your contract request form.
- Press the ‘Get Form’ button to access the contract request form and open it for editing.
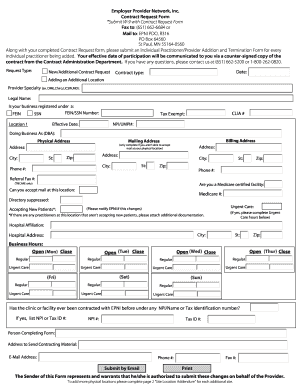
- Begin filling out the general information section, indicating the request type (e.g., new or additional contract) and the date on which you are submitting the form.
- Specify the contract type, set the effective date of participation, and enter the provider specialty (for example, Durable Medical Equipment, Chiropractic, Licensed Independent Clinical Social Worker, or Medical Doctor).
- Provide the legal name of your business. Indicate whether your business is registered under a Federal Employer Identification Number (FEIN) or a Social Security Number (SSN). Include the respective number and the National Provider Identifier (NPI) or Unique Medicaid Provider Identifier (UMPI), if applicable.
- For Location 1, fill in the required information including the CLIA number (if applicable), tax exemption status, Doing Business As (DBA) name, and the physical address.
- Complete the billing address section only if you cannot accept mail at the physical location. Provide the address, city, state, and zip code.
- Fill out the referral fax number if applicable, and indicate if you are a Medicare certified facility and if you can accept mail at this location. Include your Medicare number if you have one.
- Indicate if you are accepting new patients and provide urgent care hours if applicable. If any practitioners at this location are not accepting new patients, be sure to attach additional documentation.
- Complete the hospital affiliation details if relevant, including the name and address of the hospital.
- Fill in the business hours for both regular and urgent care services, specifying the open and close times for each day as needed.
- If applicable, complete additional sections for more physical locations by filling out the Site Location Addendum for each site.
- After completing the form, submit it by email, or choose to print it for mailing or faxing. Ensure all fields are filled correctly before submission.
Start completing your Employer Provider Network Inc contract request form online today!
Add an image to a document or presentation On your computer, open a document or presentation in Google Docs or Slides. Click Insert. Image. Choose where to get your image from. Upload from computer: Insert an image saved on your device. Search the web: Search the web for an image. ... Click Insert or Open.