Loading
Get Compensation Form
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the Compensation Form online
This guide provides clear and detailed instructions on how to complete the Compensation Form online. By following these steps, users can effectively submit the necessary information regarding an employee's death or incapacity due to occupational disease.
Follow the steps to complete the form accurately.
- Press the ‘Get Form’ button to access the Compensation Form and open it in your preferred online editor.
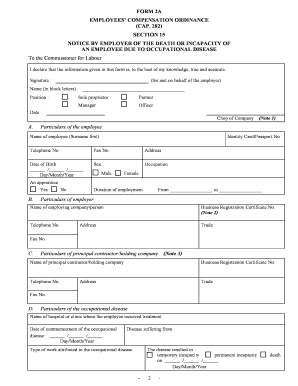
- Begin with Section A, where you will enter the particulars of the employee. Please provide the employee's full name, identity card or passport number, telephone number, and address. Ensure the date of birth is formatted as day/month/year and the sex choice is correctly indicated.
- In Section A, also indicate the employee's occupation and confirm whether they were an apprentice by selecting 'yes' or 'no'.
- In Section B, fill in the particulars of the employer, including the name of the employing company or individual, business registration certificate number, telephone number, trade, address, and fax number.
- Proceed to Section C if applicable, which requires details of the principal contractor or holding company. Include the name, business registration certificate number, telephone number, trade, address, and fax number.
- In Section D, provide details of the occupational disease. Input the name of the hospital or clinic where the employee received treatment, the date the disease started, the name of the disease, and the type of work that contributed to this condition. Additionally, specify if the disease resulted in temporary incapacity, permanent incapacity, or death.
- Fill out Section E with the insurance details, including the policy number and the name and address of the insurance company at the time of the employee’s incapacity or death.
- Section F focuses on the earnings of the employee. Choose whether rest days are paid or not and indicate the average number of working days per month. Provide the details of basic salary, food allowances, and any other earnings for the month preceding incapacity or death.
- If applicable, complete Section G regarding the fatal case, including whether police were notified, the name and address of the next-of-kin, and the relationship to the deceased.
- For temporary incapacity cases that qualify for direct settlement, fill in Section H with the period of sick leave and the amount of compensation. Finally, add the total number of sick leave days taken.
- Once all sections are completed, remember to provide your signature (for and on behalf of the employer), name in block letters, position, and the date. The company chop must be affixed in both copies of the form.
- Review the filled form carefully for accuracy. Once satisfied, save the changes, download the document, print it for your records, or share it as necessary.
Complete your documents online today for efficient processing!
OhioBWC - Common - Form: (C-240) - Introduction. Settlement Agreement and Application for Approval of Settlement Agreement. (C-240) Introduction. A settlement is an agreement between the employer, the injured worker, and BWC for a specific amount of money to settle one or more claims.
Industry-leading security and compliance
US Legal Forms protects your data by complying with industry-specific security standards.
-
In businnes since 199725+ years providing professional legal documents.
-
Accredited businessGuarantees that a business meets BBB accreditation standards in the US and Canada.
-
Secured by BraintreeValidated Level 1 PCI DSS compliant payment gateway that accepts most major credit and debit card brands from across the globe.