Loading
Get Ca.doc. First Report Of Injury Or Illness
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to use or fill out the CA.doc. First Report Of Injury Or Illness online
Filling out the CA.doc. First Report Of Injury Or Illness is an essential process for employers in California to report workplace injuries or illnesses. This guide provides clear, step-by-step instructions to help you complete this form accurately and efficiently.
Follow the steps to fill out the CA.doc. First Report Of Injury Or Illness online.
- Click the ‘Get Form’ button to obtain the form and open it in the online editor.
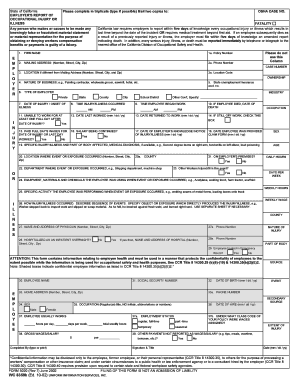
- Enter the firm name and policy number in the designated fields. Ensure that this information is current and accurately reflects the employer's details.
- Provide the mailing address, including the number, street, city, and zip code. This should be where official correspondence can be sent.
- Fill in the phone number associated with the employer for contact purposes.
- If the workplace location differs from the mailing address, enter it in the specified section along with the location code.
- Indicate the nature of the business, giving a brief description to provide context about the work environment.
- Fill in the state unemployment insurance account number for reference.
- Select the type of employer by checking the appropriate box corresponding to private, state, county, city, or other government entities.
- Document the date of injury or onset of illness using the specified format (mm/dd/yy).
- Record the time the injury or illness occurred, ensuring accuracy for legal documentation.
- Confirm if the employee was unable to work for at least one full day after the incident by checking the corresponding box.
- Provide the date the employee last worked before the injury or illness occurred.
- If applicable, enter the date of death if it occurred due to the reported injury or illness.
- Indicate the date the employee returned to work, or check the box if they are still off work.
- State whether full day's wages were paid for the date of the injury or the last day worked.
- Specify if the salary is being continued during the employee's absence from work.
- Record the date the employer became aware of the injury or illness.
- Enter the date the employee was provided with the claim form.
- Describe the specific injury or illness and the affected part of the body, including a medical diagnosis if available.
- Document the location where the event or exposure that caused the injury or illness occurred.
- Confirm if the incident took place on the employer's premises by selecting yes or no.
- Specify the department where the event or exposure happened.
- Indicate if other workers were injured or ill in the same event.
- List the equipment, materials, and chemicals the employee was using at the time of the incident.
- Detail the specific activity the employee was performing when the incident occurred.
- Provide a description of how the injury or illness occurred, including the sequence of events and any objects or exposures involved.
- Enter the name and address of the physician treating the employee, along with their contact number.
- Specify if the employee was hospitalized as an inpatient overnight and provide the name and address of the hospital if applicable.
- Indicate if the employee was treated in the emergency room.
- Complete the employee's personal information fields, including their name, social security number, date of birth, home address, and phone number.
- Include the employee's occupation without using initials, abbreviations, or numbers.
- Record the date of hire for the employee.
- Fill in the employment status (e.g., full-time, part-time, temporary, or seasonal).
- State the gross wages or salary of the employee.
- Complete any other payments that have not been reported as wages or salary.
- Provide a signature and title of the person completing the form, along with the completion date.
- Review all entries for accuracy before saving the form.
- Once completed, save changes, download, print, or share the form as necessary.
Complete the CA.doc. First Report Of Injury Or Illness online today to ensure compliance and proper reporting!
OBTAIN first aid or other necessary medical treatment as soon as possible. ... NOTIFY your supervisor about the injury and the way in which it occurred, as soon as possible. ... COMPLETE a claim for workers' compensation on Form C-3 and mail it to the nearest office of the Workers' Compensation Board, if there is lost-time.
Industry-leading security and compliance
US Legal Forms protects your data by complying with industry-specific security standards.
-
In businnes since 199725+ years providing professional legal documents.
-
Accredited businessGuarantees that a business meets BBB accreditation standards in the US and Canada.
-
Secured by BraintreeValidated Level 1 PCI DSS compliant payment gateway that accepts most major credit and debit card brands from across the globe.