Loading
Get Employment Data Form
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the Employment Data Form online
Filling out the Employment Data Form online is an important step in managing your healthcare benefits. This guide provides a clear and comprehensive walkthrough of each section of the form to ensure you complete it accurately and effectively.
Follow the steps to complete the Employment Data Form.
- Click ‘Get Form’ button to obtain the form and open it in your browser.
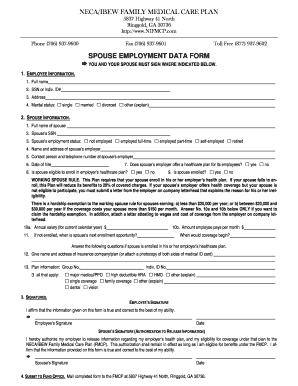
- Begin by entering your personal information in the employee information section. This includes your full name, social security number or individual ID number, mailing address, and marital status.
- Proceed to the spouse information section. Enter your spouse's full name, social security number, and current employment status. Make sure to specify whether they are not employed, employed full-time, part-time, self-employed, or retired.
- Fill in your spouse's employer details, including the name and address of their employer, along with a contact person's name and telephone number.
- Note the date of hire for your spouse in the provided field.
- Answer the questions regarding your spouse’s eligibility for their employer’s healthcare plan, including whether the plan is offered, if your spouse is eligible to enroll, and if they are currently enrolled.
- If your spouse is not enrolled and you wish to claim a hardship exemption, input the annual salary and the amount they pay per month, and provide details regarding the next enrollment opportunity and when coverage would begin.
- Should your spouse be enrolled in their employer’s healthcare plan, provide the name and address of the insurance company or attach a photocopy of their medical ID card. Also, fill in the group number and indicate the types of coverage applicable.
- Ensure both you and your spouse sign the form where indicated, affirming that the information is true to the best of your knowledge.
- Submit the completed form by mailing it to the FMCP at 5837 Highway 41 North, Ringgold, GA 30736.
Start filling out your Employment Data Form online today to ensure timely processing of your healthcare benefits.
What kind of details should an employee information form contain? Full name. Address and phone number. Social Security Number (SSN). Spouse information. Position and department. Start date. Salary. Emergency contact information.
Industry-leading security and compliance
US Legal Forms protects your data by complying with industry-specific security standards.
-
In businnes since 199725+ years providing professional legal documents.
-
Accredited businessGuarantees that a business meets BBB accreditation standards in the US and Canada.
-
Secured by BraintreeValidated Level 1 PCI DSS compliant payment gateway that accepts most major credit and debit card brands from across the globe.