Loading
Get Pds Change Of Address Form - Highmark Blue Shield
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the PDS Change Of Address Form - Highmark Blue Shield online
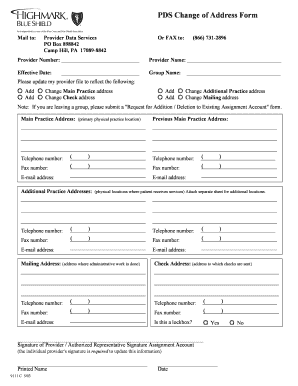
The PDS Change Of Address Form is an important document that allows providers to update their address information with Highmark Blue Shield. Filling out this form correctly ensures that accurate information is maintained in the provider’s file.
Follow the steps to complete the form accurately.
- Click ‘Get Form’ button to obtain the form and open it in the online editor.
- Begin by entering the provider number in the designated field. This number is essential for identification purposes.
- Fill in the provider name. Ensure it matches the information on record with Highmark Blue Shield for consistency.
- Specify the effective date of the address change. This date indicates when the new address should be recognized.
- Complete the group name field if applicable. This is necessary for group practices managing multiple providers.
- Indicate the type of address change by checking the appropriate options such as adding or changing the main practice address, check address, additional practice address, or mailing address.
- Enter the main practice address in the provided section, ensuring it reflects the most current location.
- Should you be updating from a previous main practice address, ensure to provide that information as well.
- List the primary telephone and fax numbers associated with the main practice address. Include area codes.
- Fill in the email address for the main practice where communication will be directed.
- For additional practice addresses, repeat the similarly structured fields including contact numbers and email as necessary. Attach a separate sheet if there are more than two additional addresses.
- Provide the mailing address, which should be where administrative tasks are managed, along with the corresponding contact information.
- Complete the check address section to specify where payments should be sent.
- Indicate whether the check address is a lockbox by selecting yes or no.
- Ensure a signature is provided by the provider or an authorized representative along with their printed name and date to validate the changes.
- Once all fields are filled out, review the form for accuracy and completeness, then save changes, download, print, or share the form as needed.
Take action now and ensure your provider information is updated online.
Return the completed Claim Form to: Highmark Blue Cross Blue Shield, the Claims Administrator for the medical component of the Plan, at the following address: Highmark Blue Cross Blue Shield P. O. Box 1210 Pittsburgh, PA 15230-1210 • Attach: all original itemized bills to the claim form.
Industry-leading security and compliance
US Legal Forms protects your data by complying with industry-specific security standards.
-
In businnes since 199725+ years providing professional legal documents.
-
Accredited businessGuarantees that a business meets BBB accreditation standards in the US and Canada.
-
Secured by BraintreeValidated Level 1 PCI DSS compliant payment gateway that accepts most major credit and debit card brands from across the globe.