Loading
Get 2017 Claim Form Filled Out
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the 2017 Claim Form Filled Out online
Filling out the 2017 Claim Form Filled Out online can streamline your submission process and ensure that all necessary information is accurately provided. This guide offers step-by-step instructions tailored to individuals who may have little experience with such forms, ensuring a smooth completion process.
Follow the steps to successfully complete the 2017 Claim Form Filled Out.
- Click ‘Get Form’ button to obtain the form and open it in the editor.
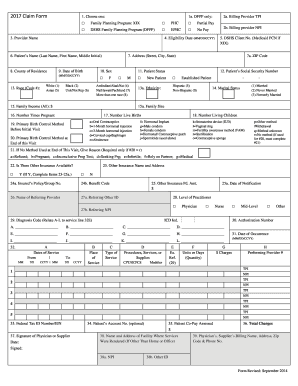
- Select the appropriate program by checking the box corresponding to the services being billed: Family Planning Program: XIX, DSHS Family Planning Program (DFPP), Primary Health Care (PHC), or Expanded Primary Health Care (EPHC).
- Input the billing provider's nine-digit TPI in the field labeled 'Billing Provider TPI.'
- Enter the billing provider's NPI in the 'Billing Provider NPI' section.
- Fill in the 'Provider Name' section with the name of the provider as enrolled.
- Indicate the eligibility date for services by entering the date in MM/DD/CCYY format.
- Provide the patient's name (Last Name, First Name, Middle Initial) as shown on their identification.
- Complete the patient's address, including street, city, and state.
- Input the ZIP code in the required field.
- Enter the county of residence for the patient.
- Input the patient's date of birth in MM/DD/CCYY format.
- Check the appropriate box to indicate the patient's sex.
- Select 'New Patient' or 'Established Patient' in the patient status section.
- Enter the patient's Social Security number. If unavailable, use 000-00-0001.
- Indicate the patient's race by entering the appropriate code number.
- Specify the patient's ethnicity by entering the relevant code.
- Indicate the marital status by entering the appropriate marital code.
- Input the family's total gross monthly income.
- Provide the family size relevant to the reported income.
- Indicate the number of times the patient has been pregnant.
- Input the number of live births experienced by the patient.
- Enter the number of living children this patient has.
- Fill out the primary birth control method used before the initial visit.
- Indicate the primary birth control method at the end of the visit.
- If no method was used at the end of the visit, provide a reason.
- Indicate if other insurance is available by checking 'Yes' or 'No.'
- If applicable, provide the other insurance name and address.
- Input the insured’s policy/group number.
- Fill in the benefit code if applicable.
- Enter the amount paid by other insurance if applicable.
- Input the date of notification for the other insurance payment or denial.
- If relevant, include the name of the referring provider.
- Provide the referring provider's NPI if necessary.
- Enter the level of practitioner who provided the service.
- Input the diagnosis code as required.
- Provide the authorization number, if applicable.
- Enter the date of occurrence related to the claims.
- Fill out the dates of service, ensuring each date is in MM/DD/CCYY format.
- Specify the place of service using the appropriate POS code.
- Enter procedures, services, or supplies using the appropriate CPT/HCPCS code.
- Relate the diagnosis codes to the services provided.
- Indicate the number of units or days charged.
- Fill out the charges for each listed service.
- Provide the performing provider's TPI and NPI information.
- If necessary, input the federal tax ID number (EIN).
- Enter the patient's account number, if applicable.
- Specify any patient copay assessed.
- Sum up the total charges for the claim.
- Ensure the claim is signed and dated by the physician or supplier.
- Enter the name and address of the facility where services were rendered, if applicable.
- Include the physician’s or supplier’s billing name and contact details.
Begin filling out your documents online to ensure a smooth submission process.
Other CMS-1500 Codes Y4. Property Casualty Claim Number. 431. Onset of Current Symptoms or Illness. 484. ... 454. Initial Treatment. 304. ... DN. Referring Provider. DK. ... 0B. State License Number. 1G. ... ICD-9-CM. ICD-10-CM. Replacement of prior claim. Void/cancel of prior claim. AV. Available – Not Used (Patient refused referral.) S2.
Industry-leading security and compliance
US Legal Forms protects your data by complying with industry-specific security standards.
-
In businnes since 199725+ years providing professional legal documents.
-
Accredited businessGuarantees that a business meets BBB accreditation standards in the US and Canada.
-
Secured by BraintreeValidated Level 1 PCI DSS compliant payment gateway that accepts most major credit and debit card brands from across the globe.