Loading
Get Fillable F00039
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the Fillable F00039 online
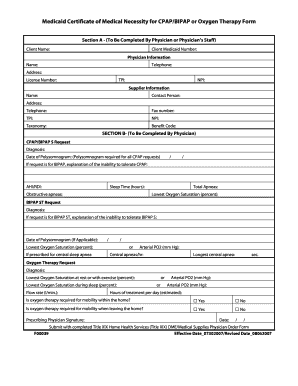
Filling out the Fillable F00039 form is a crucial step for obtaining Medicaid coverage for medical necessities such as CPAP/BIPAP or oxygen therapy. This guide will provide you with clear instructions on completing the form to ensure that you submit accurate and complete information.
Follow the steps to successfully complete the Fillable F00039 form.
- Click ‘Get Form’ button to acquire the form and open it in your preferred PDF editor.
- Begin completing Section A, which should be filled out by the physician or their staff. Input the client’s name and Medicaid number. Then, provide the physician's information, including their name, telephone number, address, license number, TPI, and NPI.
- Provide supplier information, detailing the name, contact person, address, telephone, fax number, TPI, NPI, taxonomy, and benefit code.
- Move to Section B, where the physician will fill out the specific request for CPAP/BIPAP S or BIPAP ST. Include the diagnosis, date of the polysomnogram, and pertinent details such as AHI/RDI, sleep time, obstructive apneas, total apneas, and the lowest oxygen saturation percentage.
- If BIPAP is requested, provide a detailed explanation of the inability to tolerate CPAP when necessary. Fill in details relevant to the BIPAP ST request, including a justification for the prescription and relevant polysomnogram data.
- For oxygen therapy requests, specify the diagnosis, lowest oxygen saturation at rest and during sleep, flow rate, and whether oxygen therapy is required for mobility both within and outside the home.
- The prescribing physician must sign the form, include the date, and make sure to submit it along with a completed Title XIX Home Health Services DME/Medical Supplies Physician Order Form.
- After completing the form, save your changes. You can then download, print, or share the completed document as needed.
Complete your Medicaid forms online with ease and ensure accurate information submission.