Loading
Get Healthpartners Coordination Of Benefits Form
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the Healthpartners Coordination Of Benefits Form online
Filling out the Healthpartners Coordination Of Benefits Form can help ensure that your claims are processed efficiently. This guide provides a step-by-step overview to assist you in completing the form correctly and submitting it online.
Follow the steps to fill out the form accurately.
- Click ‘Get Form’ button to obtain the form and open it in the editor.
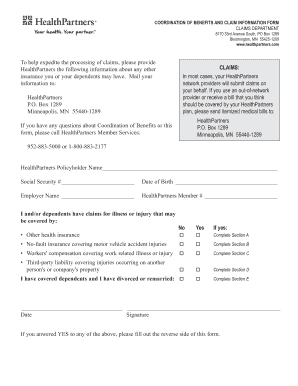
- Begin by entering the Healthpartners policyholder's name, social security number, and date of birth in the designated fields.
- Next, fill in the employer's name and your Healthpartners member number. Make sure this information is accurate to avoid any processing delays.
- Indicate whether you or your dependents have claims for illness or injury that may be covered by other insurance by selecting 'Yes' or 'No'. If you select 'Yes', you will need to complete the relevant sections that pertain to the type of other coverage.
- If applicable, complete Section A for other health insurance information. Provide the name of the other insurance policyholder, their date of birth, the name of the insurance company, their contact address, and policy/group number. Indicate the type of coverage, either single or family.
- If you are completing Section B, provide details for no-fault insurance, including the name of the affected family member, the date of the original injury, and a description of the injury. Also, fill in the auto insurance carrier’s details.
- For Section C related to workers' compensation, provide the name of the affected family member, the date of the injury, and their employer's name along with relevant carrier details.
- In Section D, enter information for third-party liability covering injuries, including the name of the affected family member and financial responsible party's details.
- If applicable, complete Section E if you are divorced or remarried and have dependents. List the child's complete name, the names of those with legal custody, and healthcare expense responsibilities.
- Once all sections are filled out, review the information for accuracy. You can then save your changes, download the form, print it, or share it as needed.
Start filling out your Healthpartners Coordination Of Benefits Form online today.
All Rights Reserved. You keep all rights to your material. This is by far the most commonly used and seen statement of rights in copyrighted materials.
Industry-leading security and compliance
US Legal Forms protects your data by complying with industry-specific security standards.
-
In businnes since 199725+ years providing professional legal documents.
-
Accredited businessGuarantees that a business meets BBB accreditation standards in the US and Canada.
-
Secured by BraintreeValidated Level 1 PCI DSS compliant payment gateway that accepts most major credit and debit card brands from across the globe.