Loading
Get Ime Medicare Crossover Invoice Form
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the Ime Medicare Crossover Invoice Form online
Navigating the Ime Medicare Crossover Invoice Form can be straightforward with the right guidance. This guide provides detailed, step-by-step instructions on how to effectively complete each section of the form online, ensuring that your submission is accurate and efficient.
Follow the steps to complete the form accurately
- Click the ‘Get Form’ button to obtain the Ime Medicare Crossover Invoice Form and open it in your preferred digital editor.
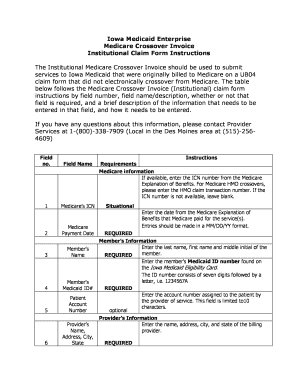
- Begin by entering Medicare's Internal Control Number (ICN) in field 1 if available. If not, leave this field blank.
- Enter the Medicare payment date in field 2. Use the format MM/DD/YY for accurate submission.
- In field 3, input the member's name using the last name, first name, and middle initial.
- Provide the member's Medicaid ID number in field 4, which can be found on their Iowa Medicaid Eligibility Card.
- For field 5, enter the patient account number assigned by the service provider. This is an optional field, but the length must not exceed 10 characters.
- Input the billing provider’s name, address, city, and state in field 6, ensuring all elements of the address are included.
- Enter the zip code associated with the billing provider in field 7.
- In field 8, provide the National Provider Identifier (NPI) for the billing provider.
- Enter the provider's taxonomy code in field 9.
- For field 10, check the box if the member has other insurance coverage beside Medicare and Medicaid.
- If other insurance has denied coverage, indicate this in field 11 by checking the respective box.
- In field 12, report any amount paid by the other insurance, if applicable.
- Input the primary diagnosis code in field 13, following ICD-9-CM guidelines.
- If there are other diagnosis codes, provide them in fields 14-18 as needed, ensuring the ICD-9-CM format is used.
- Enter the type of bill in field 19 using the three-digit code corresponding to the service type from the Medicare Explanation of Benefits (EOB).
- Document the date(s) of service in fields 20a and 20b, reflecting the period indicated in the EOB.
- If applicable, enter the number of covered days in field 21. Ensure you do not include the day of discharge.
- Provide the total covered charges from the Medicare EOB in field 22.
- If there are any non-covered charges, enter the total in field 23.
- If indicated on the EOB, fill out fields 24 through 28 with respective amounts for the deductible, blood deductible, coinsurance, copay, and provider paid amounts.
- At the end of the form, the provider or an authorized representative must sign in field 29 and enter the original filing date in field 30.
- After completing the form, save your changes, download, print, or share the form as necessary.
Complete your documents online today to streamline your billing process.
1-888-543-6742 (Toll Free)
Industry-leading security and compliance
US Legal Forms protects your data by complying with industry-specific security standards.
-
In businnes since 199725+ years providing professional legal documents.
-
Accredited businessGuarantees that a business meets BBB accreditation standards in the US and Canada.
-
Secured by BraintreeValidated Level 1 PCI DSS compliant payment gateway that accepts most major credit and debit card brands from across the globe.