Loading
Get Medical Providers Forms Urc
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the Medical Providers Forms Urc online
This guide provides a comprehensive, step-by-step approach to filling out the Medical Providers Forms Urc online. Users can follow these instructions to ensure accurate and complete submissions.
Follow the steps to fill out the Medical Providers Forms Urc successfully.
- Click ‘Get Form’ button to obtain the form and open it in your online editor.
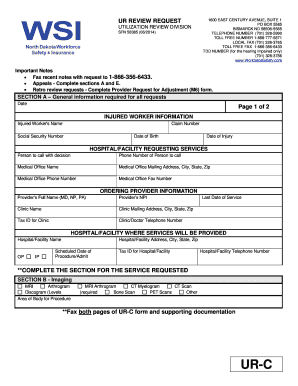
- Begin by completing Section A, which covers general information required for all requests. Fill in the injured worker's name, claim number, social security number, date of birth, and date of injury.
- Provide details for the hospital or facility requesting services, including the person's name to call with the decision, their phone number, and the medical office name and address.
- In the ordering provider information section, enter the provider's full name, NPI, clinic name, mailing address, tax ID, telephone number, and the last date of service.
- Complete the hospital or facility information section where services will be provided, including the hospital name, address, scheduled date of procedure or admission, tax ID, and telephone number.
- When completing Section B for imaging services, select the required procedures and indicate the area of the body for the procedure.
- For Section C, fill in the details regarding injections, including the type of injection, specific levels if required, and the side (right, left, or bilateral).
- In Section D, provide information for therapies needed, including the area of the body, diagnosis, specific treatment requested, frequency, and the therapist's name.
- For Section E, describe any surgeries, appeals, concurrent, or other services required, and ensure to include the most recent doctor notes.
- Finally, review all entries for accuracy, then save changes. You can download, print, or share the completed form as needed.
Complete the Medical Providers Forms Urc online today for efficient processing of your request.
Documents to be submitted: Duly completed claim form. Photo Identity proof of the patient. Medical practitioner's prescription advising admission. Original bills with itemized break up. Payment receipts. Discharge summary including complete medical history of the patient along with other details.