Loading
Get D-8 - Form - Employer's Wage Verification Form
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the D-8 - Form - Employer's Wage Verification Form online
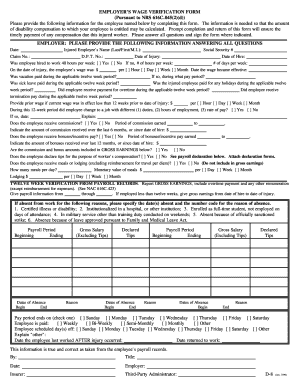
Filling out the D-8 - Form - Employer's Wage Verification Form is essential for calculating the disability compensation entitled to an injured employee. This guide provides a step-by-step process to complete the form accurately and promptly online.
Follow the steps to fill out the D-8 - Form online.
- Press the ‘Get Form’ button to access the D-8 - Form and open it on your device.
- Enter the date at the top of the form, ensuring it reflects the current date or the date the form is being filled out.
- Provide the injured employee's name, including their last name, first name, and middle initial in the designated fields.
- Fill in the claim number and D.P.T. number associated with the employee's case.
- Input the employee's Social Security number to maintain identification accuracy.
- Record the date of the injury and the employee's date of hire in the specified sections.
- Indicate whether the employee was hired to work 40 hours per week. If not, specify the actual number of hours worked per week.
- Provide the employee's wage on the date of injury and specify how often they are paid (hourly, daily, weekly, or monthly) along with the date when this wage became effective.
- Answer questions regarding vacation pay, sick leave, holiday pay, overtime payment, and termination pay during the applicable twelve-week period.
- If applicable, fill in the prior wage information for the employee if the current wage was effective for less than 12 weeks prior to the injury date.
- State whether the employee changed jobs or received commissions or bonuses, along with the related earnings and periods.
- List any absences during the last twelve weeks and detail the reasons for those absences, including relevant dates.
- After completing the form, review all fields for accuracy and sign where indicated, entering your title and the date.
- Once all information is filled in, save your changes, and you can choose to download, print, or share the completed form.
Complete the D-8 - Form - Employer's Wage Verification Form online today for timely compensation processing.
Workers' compensation, a no-fault insurance plan, provides guaranteed financial payments for work related injuries and illnesses. Financial compensation includes lost wages (i.e. temporary disability payments), medical bills, and lump sum permanent disability payments.
Industry-leading security and compliance
US Legal Forms protects your data by complying with industry-specific security standards.
-
In businnes since 199725+ years providing professional legal documents.
-
Accredited businessGuarantees that a business meets BBB accreditation standards in the US and Canada.
-
Secured by BraintreeValidated Level 1 PCI DSS compliant payment gateway that accepts most major credit and debit card brands from across the globe.