Get Dhcs 9116
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the Dhcs 9116 online
Filling out the Dhcs 9116 online is a straightforward process that ensures you provide all necessary information accurately. This guide aims to support users in completing the form correctly, helping to facilitate timely payment and compliance with requirements.
Follow the steps to complete the Dhcs 9116 form online.
- Click ‘Get Form’ button to obtain the form and open it in the editor.
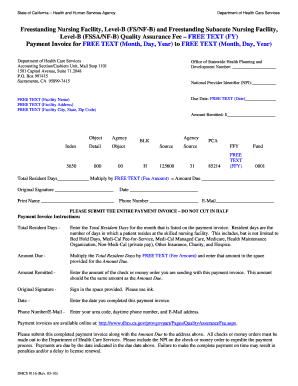
- Start by entering the facility name in the designated field labeled 'Facility Name.' This should reflect the official name of your nursing facility.
- Proceed to fill in the 'Facility Address' with the complete street address of your facility, ensuring all details are accurate to avoid delays.
- Next, enter the city, state, and zip code in the respective fields to accurately reflect your facility's location.
- Indicate the 'Due Date' in the specified format, ensuring you meet all deadlines to avoid penalties.
- Enter your National Provider Identifier (NPI) number in the corresponding field. This is vital for proper identification and processing.
- Calculate the 'Total Resident Days' for the month indicated on your payment invoice. This includes all days that residents have occupied beds, including those covered by various insurance types.
- Multiply the 'Total Resident Days' by the predetermined fee amount to determine the 'Amount Due.' Enter this figure in the allotted space.
- Fill in the 'Amount Remitted,' which should match the 'Amount Due' that you calculated earlier.
- Provide an original signature in the designated area using ink. This is required for the form to be valid.
- Complete the date field with the date you are finalizing this payment invoice.
- Finally, include your daytime phone number and email address to ensure that you can be contacted if necessary.
- After reviewing all details for accuracy, you can save the changes made to the form, download it, print it for physical submission, or share it as needed.
Complete your Dhcs 9116 form online today to streamline your submission process!
To request a Medi-Cal exemption from DHCS, you need to complete the necessary forms and submit them to the Department of Health Care Services. First, gather all required documentation to support your request. Then, visit the official DHCS website to find the specific forms related to exemption requests under Dhcs 9116. After completing the forms, submit them through the designated channels mentioned on the site, and be sure to keep a copy for your records.