Loading
Get Form 5 Wc
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the Form 5 Wc online
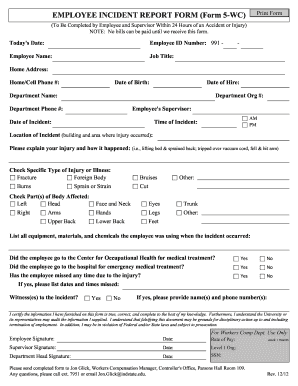
Filling out the Form 5 Wc online is an essential step for reporting workplace incidents. This guide provides clear instructions to help you complete the form accurately and efficiently.
Follow the steps to fill out the Form 5 Wc online.
- Click ‘Get Form’ button to access the form and open it in your preferred digital editor.
- Enter today's date in the designated field to provide a record of when the form was filled out.
- Fill in your employee ID number and full name in the corresponding fields.
- Specify your job title and complete your home address, including street, city, state, and zip code.
- Provide your home or cell phone number to facilitate further communication.
- Enter your date of birth and date of hire to give a complete background on your employment.
- Fill in your department name, organization number, and department phone number for proper tracking of the incident.
- Indicate the name of your supervisor responsible for overseeing your work.
- Record the date and time of the incident, using AM or PM to clarify the specifics.
- Describe the location of the incident in detail, mentioning the specific building and area where it took place.
- Provide a clear explanation of your injury and describe how it occurred, using illustrative examples if necessary.
- Select the specific type of injury or illness from the provided checkboxes.
- Indicate the parts of the body that were affected by the incident by selecting the relevant options.
- List all equipment, materials, and chemicals that you were using at the time of the incident.
- Answer the questions regarding medical treatment, indicating if you visited the Center for Occupational Health or a hospital.
- If applicable, provide details about any time missed from work due to the injury, including specific dates and times.
- Identify any witnesses to the incident, and if there are any, provide their names and phone numbers.
- Sign the form to certify that the information provided is accurate and understand the implications of falsifying information.
- Ensure your supervisor and department head sign the document as required.
- Once completed, save your changes, and you can download, print, or share the form as necessary.
Complete your documents and file the Form 5 Wc online today.
Related links form
When you talk to an insurance adjuster, avoid making vague comments or over-explaining your situation. Stick to the facts presented in Form 5 Wc and refrain from discussing any previous injuries or health issues that are unrelated to your current claim. This approach protects your interests and helps maintain the clarity of your case.