Loading
Get Complete Section A Policyholderpatient Information And Sign Your Claim Form
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the Complete Section A Policyholder/Patient Information And Sign Your Claim Form online
Completing the Complete Section A Policyholder/Patient Information and Sign Your Claim Form online is an essential step in processing your claim efficiently. This guide provides clear, step-by-step instructions to help you accurately fill out each component of the form.
Follow the steps to successfully complete your claim form.
- Click ‘Get Form’ button to obtain the form and open it in the editor.
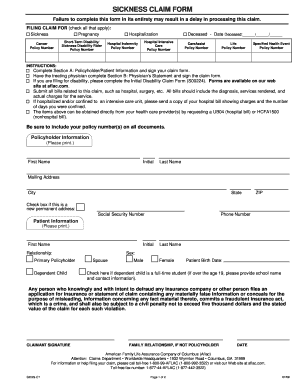
- In the first section titled 'Policyholder Information,' enter your first name, initial, and last name. Complete the mailing address, including city, state, and ZIP code. If this is a new permanent address, check the designated box.
- Provide your Social Security Number and phone number in the specified fields.
- Next, move to the 'Patient Information' section. Enter the patient’s first name, initial, and last name.
- Indicate the relationship of the patient to the policyholder by selecting the appropriate option (Primary Policyholder, Spouse, or Dependent Child).
- Select the patient's sex by checking 'Male' or 'Female' and enter the patient’s birth date.
- If the dependent child is a full-time student, check the box and provide the school name and contact information, if applicable.
- Review the ‘Claimant Signature’ section. As the claimant, sign the form, indicate family relationship if you are not the policyholder, and enter the date of your signature.
- After completing the form, review all entries for accuracy. Save your changes, and you will have the option to download, print, or share the form as needed.
Complete your documents online today to ensure timely processing of your claim.
The patient registration form should include the patient's full name, date of birth, contact information, and insurance details. It's important to capture this information accurately to avoid delays in processing claims. Including these details allows healthcare providers to complete Section A PolicyholderPatient Information And Sign Your Claim Form efficiently.
Industry-leading security and compliance
US Legal Forms protects your data by complying with industry-specific security standards.
-
In businnes since 199725+ years providing professional legal documents.
-
Accredited businessGuarantees that a business meets BBB accreditation standards in the US and Canada.
-
Secured by BraintreeValidated Level 1 PCI DSS compliant payment gateway that accepts most major credit and debit card brands from across the globe.