Loading
Get Fmla Certification Form
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the Fmla Certification Form online
The Fmla Certification Form is a critical document that helps employees request leave under the Family and Medical Leave Act. This guide provides a step-by-step approach to filling out the form online, ensuring users understand each section and can submit the required information effectively.
Follow the steps to complete the Fmla Certification Form online
- Click ‘Get Form’ button to obtain the form and open it in your preferred editor.
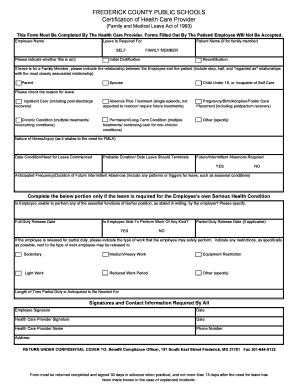
- Begin by filling in the employee's name in the designated field at the top of the form.
- Next, indicate whether the leave is required for the employee themselves or for a family member.
- If the leave is for a family member, specify the relationship between the employee and the patient, including options like parent, spouse, and child.
- Choose whether this submission is an initial certification or a recertification by selecting the appropriate option.
- Check the reason for the leave from the provided list, such as inpatient care or chronic condition.
- Detail the nature of the illness or injury that necessitates the leave.
- Input the date when the condition or need for leave commenced, as well as the probable duration of the leave.
- Indicate whether future intermittent absences are required and provide information on their anticipated frequency and duration.
- If the leave is for the employee's serious health condition, specify if they are unable to perform essential job functions.
- Indicate the full duty release date, or any partial duty release details if applicable, and describe any work restrictions.
- Provide the length of time partial duty is anticipated to be needed for.
- Ensure all required signatures are filled in, including the employee's and the health care provider's, along with their names, phone numbers, and addresses.
- Once completed, review all entries for accuracy, then save changes, download, print, or share the form as needed.
Complete your Fmla Certification Form online to ensure a smooth leave request process.
Related links form
Employers typically verify FMLA claims through the documentation provided, particularly the Fmla Certification Form filled out by your healthcare provider. They may also reach out to your doctor for clarification or additional information regarding your medical needs. It is crucial to submit accurate and detailed documentation to facilitate the verification process.