Loading
Get Dhcs 4493 Form
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the Dhcs 4493 Form online
This guide provides a clear and user-friendly overview of how to fill out the Dhcs 4493 Form online. It offers step-by-step instructions to assist users in completing the form accurately and efficiently.
Follow the steps to complete the Dhcs 4493 Form online.
- Click the ‘Get Form’ button to obtain the Dhcs 4493 Form and open it in the editor.
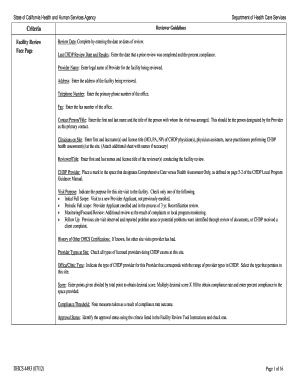
- Enter the review date in the designated field. Make sure to input the correct date or dates pertaining to the review.
- Provide the date of the last Child Health and Disability Prevention (CHDP) review and its compliance percent in the respective field.
- Fill in the legal name of the provider for the facility being reviewed in the provider name section.
- Enter the complete address of the facility under the address section, ensuring accuracy for verification purposes.
- Input the primary phone number of the office in the telephone number field.
- If applicable, fill in the fax number of the office in the designated fax field.
- Provide the first and last name of the contact person, along with their title, in the contact person/title section.
- List the first and last name(s) and license title of CHDP physician(s), physician assistants, or nurse practitioners performing health assessments at the site in the clinicians on site section.
- Input the first and last names and license title of the reviewer(s) in the reviewer/title section.
- Indicate whether the provider is delivering Comprehensive Care or Health Assessment Only by marking the appropriate space provided.
- Select the purpose of the site visit from the options provided, ensuring to choose only one option.
- If known, list any other DHCS certifications the provider has had under the history of other DHCS certifications section.
- Select all license types of providers performing CHDP exams at the site in the provider types at site section.
- Indicate the type of CHDP provider by selecting from the office/clinic type options available.
- Calculate the compliance rate by entering the points allocated divided by the total points and multiplying by 100 to get the percent compliance, which should be entered in the score section.
- In the compliance threshold section, note any measures taken based on the compliance rate outcome.
- Identify the approval status using the criteria provided and mark one in the approval status section.
- Once all sections are completed, review the form for errors before saving changes, downloading, printing, or sharing it as necessary.
Start completing the Dhcs 4493 Form online today for a seamless review process.
California DHCs insurance refers to the comprehensive health coverage options available under the state’s Medicaid program, known as Medi-Cal. This insurance provides a wide range of services including doctor visits, hospital care, and prescription medications. To access these benefits, you may need to complete the Dhcs 4493 Form, which helps determine your eligibility and ensures you take full advantage of what California DHCs has to offer.